A Case Report of an Elderly Patient with Psoriasis Treated with Jeongri-tang Gagam-bang: Focus on Digestive System Treatment
Article information

Abstract
Objectives
This study aimed to report the efficacy of Korean medicine with Jeongri-tang Gagam-bang for treating psoriasis.
Methods
A patient with psoriasis was treated with Jeongri-tang Gagam-bang (正理湯加減方). Moreover, acupuncture was performed on CV12 (中脘) and both sides of ST25 (百會), GV20 (百會), LI4 (合谷), and LR3 (太衝) for 15 minutes. Psoriasis severity was assessed using the Psoriasis Area and Severity Index (PASI). Pruritis and dyspepsia intensities were ranked on a Visual Analog Scale (VAS) of 0–10.
Results
After treatment, the PASI changed from 21.6 to 1.6. Patient’s pruritus had almost disappeared and dyspepsia had improved.
Conclusions
This study shows that Jeongri-tang Gagam-bang (正理湯加減方) and acupuncture on CV12 (天樞), ST25 (天樞), GV20 (百會), LI4 (合谷), and LR3 (太衝) might be helpful to treat psoriasis symptoms by improving digestive function.
Introduction
Psoriasis is a skin disease characterized by red plaques, papules, silver scales, and scabs that occur locally or across the entire body. Modern Western medicine considers psoriasis an overgrowth of epidermal cells due to an imbalance of anti-inflammatory and pro-inflammatory cytokines, vascular proliferation, immune cell infiltration, and abnormal keratinocyte differentiation and proliferation. Therefore, Western medicine defines psoriasis as an autoimmune skin disease and a chronic inflammatory condition1). Psoriasis is an incurable disease with a high relapse rate and a lifelong course of exacerbations and flare-ups. Its cause remains unclear and a standardized treatment that is both effective and safe is lacking.
The treatment of psoriasis in Western medicine can be summarized as topical, systemic, phototherapy and biologics. Dermatologists treat milder cases of psoriasis with topical immunosuppressants and steroids. And more severe cases with a systemic treatment, including ultraviolet light therapy, anti-inflammatory and immunosuppressive agents, rather than a single medication. Phototherapy options include anthralin phototherapy and Psoralen Ultraviolet A (PUVA) therapy, but side effects such as nausea, headache, and dizziness have been reported, as well as the risk of skin cancer. Systemic treatments include steroids, retinoids, cyclosporine, and methotrexate. However, the long-term use of these synthetic drugs can feature side effects such as cold sores, dry skin, pruritus, and liver dysfunction. Therefore, they should be used temporarily2).
In Korean medicine, psoriasis is called Baekbi (白庀), Eunseolbyeong (銀屑病), Poongseon (風 癬), Songpiseon (松皮癬), and Baekseolpoong (白 屑風)3). Oriental medicine also recognizes and treats psoriasis as being caused by Blood heat (血 熱), Blood stasis (血瘀), Blood dryness (血燥), Yang deficiency (陽虛), Stagnant heat (鬱熱), and Release exterior (發汗) disorders1). In previous studies published in Korea, patients with psoriasis were treated with Blood deficiency induced wind dryness pattern (血虛風燥) and Wind heat induced blood heat pattern (風熱血熱) prescriptions. In the Blood deficiency induced wind dryness pattern (血虛風燥), researchers have used Dangguieumjagagambang (當歸飮子加減方) and Gamiyoonbooeum (加味潤膚飮). Wind heat induced blood heat pattern (風熱血熱) patients were prescribed Bangpoontongsungsan (防風通聖 散), Baekhotanggagambang (白虎湯加減方), and Seungmagalgeumtang (升麻葛根湯)4). In addition to herbal treatments, Huanglianhaedok pharmacoacupuncture (黃蓮解毒藥鍼) and aroma ointments were used to treat psoriasis in Korean Medicine5). There have been many clinical reports on the treatment of psoriasis with TCM, but they have all focused on the skin itself, such as the color of the skin lesions and the degree of induration.
Recent epidemiologic studies of psoriasis have shown an association between psoriasis and metabolic syndrome consisting of diabetes, obesity, and hypertension. The more severe the psoriasis, the greater its association with metabolic syndrome. Improvements in metabolic syndrome are reportedly correlated with significant improvement in psoriasis lesions6). In contrast, only one study to date published in Korea focused on metabolic syndrome and lipid metabolism in psoriasis7). Therefore, this article reports a case of psoriasis cured by improving digestive system function using Professor Gil-young Yoon's Jeongri-tang Gagam-bang (正理 湯加減方). It combines the properties of Pyeongwi-san (平胃散), Leejin-tang (二陳湯), and Hyangso-san (香蘇散) which are digestive medicine. Moreover, it is a variant of Bulhwangeumjeongki-san (不換金正氣散), which is used to clean the waste in the digestive system8). To this, Lonicera japonica Thunb flos (金銀花), Cryptotympana pustulata Fabricius periostracum (蟬退), and Spirodelae polyrhiza Schleider Herba (浮萍草) were added for anti-inflammation. To date, Jeongri-tang (正理湯) has been shown to improve gastrointestinal motility in animal models9), but there are no case reports of its efficacy in skin diseases, especially psoriasis. Therefore we would like to report the skin improvement effects of Jeongri-tang Gagam-bang (正理湯加減方) on an 82-year-old psoriasis patient with a 40-year history of hypertension, diabetes, and hyperlipidemia.
Methods
1. Subjects
A patient with psoriasis visited ○○ Oriental Clinic in Cheonan, Chungcheongnam-do between March 25, 2023 and June 16, 2023. The patient complained of dyspepsia, dry mouth, and weakness and had been taking medications for hypertension, diabetes, and hyperlipidemia for 40 years.
2. Methods
1). Assessing psoriasis
The Psoriasis Area Severity Index (PASI), designed by Fredriksson and Petterson, was adopted to assess psoriasis. The PASI score is calculated by multiplying the proportion of the body affected by psoriasis (head, 10%; trunk, 30%; upper limbs, 20%; and lower limbs, 40%); psoriasis area (0–6); and the sum of each symptom (scaling, erythema, and thickness) scores including 0 (none), 1 (slight), 2 (moderate), 3 (striking), and 4 (exceptionally striking). The resulting score ranged from a minimum of 0 to a maximum of 725).
PASI score evaluations were performed three times, once per month:
2) Determining treatment efficacy
Treatment success was defined as PASI reduced by 75% or more, and treatment failure as PASI reduced by 50% or less10).
3) Determining pruritus intensity
Pruritus degree was based on the Visual Analog Scale (VAS) score, with 0 being no pruritus and 10 being the most severe pruritus since onset. Patients were asked to rate their pruritus over a 1-month period on a scale from 0 to 10.
4) Determining chronic dyspepsia intensity
Dyspepsia degree was assessed based on the VAS score, with 0 being no dyspepsia and 10 being the most severe dyspepsia since onset. Patients were asked to rate their dyspepsia symptoms once a month on a scale from 0 to 10.
3. Therapeutic interventions
1) Herbal medicine
The patient complained of dry mouth and chronic indigestion. In the past month, he has lost a little weight because he often felt weak and unable to finish his meals. He said that he passed stool every morning but could not keep it cool, his hands and feet became hot at night, and the itching of his psoriasis became worse. I diagnosed him with Spleen yin deficiency pattern (脾陰虛) and prescribed Jeongri-tang Gagam-bang (正理湯加減方) twice daily for 90 days. The prescribed formula had the following composition8) (Table 1). There was no prescription for topical ointments.
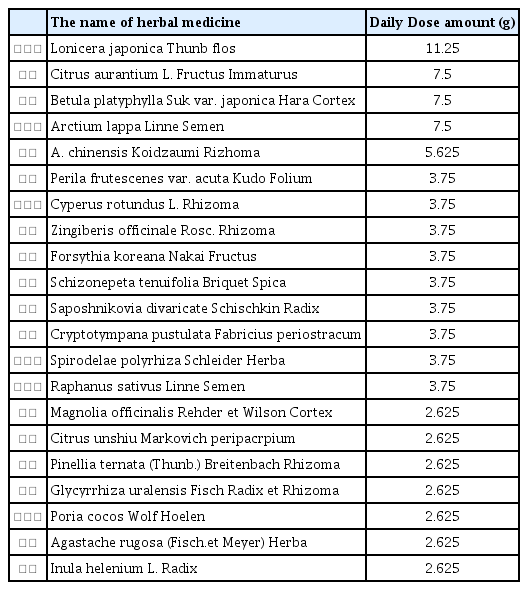
Jeongri-tang Gagam-bang prescription (正理湯加減方)
2) Acupuncture
Acupuncture treatment was performed at each weekly clinic visit. Needles were made of steriled stainless steel needles (0.20×40mm, DongBang Co. Seoul, Korea), The depth of acupuncture needles was 1–2mm per point, and acupuncture was performed on CV12 (中脘) and both sides of ST25 (天樞), GV20 (百會), LI4 (合谷), and LR3 (太衝) for 15 minutes.
3) Requirements for the diet
Restrict consumption of flour and processed foods.
Case Report
Patient: Park○○/Male/82
Chief complaint: Psoriasis (upper limb, lower limbs, trunk), nighttime pruritus, chronic dyspepsia, dry mouth, difficulty remaining asleep
Date of onset: May 2001
Present illness: In May 2001, he was diagnosed and treated for psoriasis at ○○ University Hospital. In March 2022, his symptoms worsened again, and he took oral steroids and antihistamines for 1 year as prescribed at ○○ Medical Center. At 40 days before visiting our clinic, his symptoms of weakness and indigestion worsened, and the psoriasis rapidly worsened on his stomach, trunks, and legs.
Family history: None
Past history: type 2 diabetes, hypertension, hyperlipidemia
Drinking and smoking history: None
-
Other conditions
Appetite: less than half a bowl of rice
Digestion: Frequent indigestion and bloating
Feces: Once a day but feel residual sensation
Urine: No specific condition
Tongue diagnosis: White thin coated with teeth marked dark red tongue
Sleep: Wakes up every 2 hours
Pruritus: Worsens at night
Duration of treatment: March 25, 2023, to June 16, 2023
-
Change in symptoms
Erythema color and thickness and scaling of the psoriatic lesions were recorded by PASI scores. The degrees of pruritus and dyspepsia felt by the patient were recorded as VAS scores of 0–10 (Figure 1, 2) (Tables 2, 3).

Changes in psoriasis according to treatment duration
Changes of PASI, average of pruritis VAS and average of dyspepsia VAS
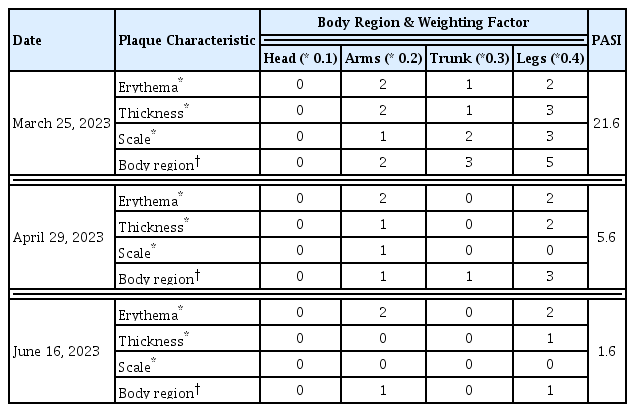
Psoriasis Area and Severity Index (PASI)
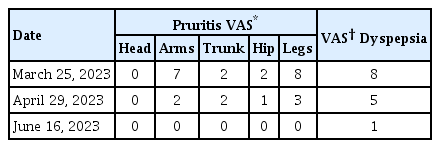
Pruritus and dyspepsia assessment using Visual Analog Scale (VAS) scores
-
March 25, 2023
-
Psoriasis condition:
Erythematous plaques of various sizes were evident. In particular, the psoriasis on the legs had a plaque-type widely distributed and thickly covered scale. The Auspitz sign was noted on the legs.
Pruritus: None during the daytime; severe at nighttime, mainly on the arms and legs
Dyspepsia: Able to eat less than half a bowl of rice at a time; felt bloated after eating and had no appetite
-
-
April 29, 2023
-
Psoriasis condition:
Only one small erythematous lesion was observed around the umbilicus. On the lower extremities, the erythematous plaque was much thinner, and its borders became blurred. New erythematous lesions were observed on the shin where a thicky plaque lesion was present. Much of the erythema on the posterior thighs had faded. On the arms, the color of the erythema was like that seen in March, but it was thinner and covered only a small portion of the skin. The erythema with silky scaling on the hips had almost disappeared, and only a few red papules remained.
Pruritus: The pruritus remained the same as in March (aggravated at night). However, the patient reported that the duration had shortened and severity had decreased. Itching was intermittent in the abdomen and hips.
Dyspepsia: He felt less bloated and was able to eat half a bowl of rice at a time.
-
-
June 16, 2023
-
Psoriasis condition:
A few small erythematous patches persisted, mostly on the right leg. Very little erythema remained on his left leg. The erythema on the lower arm was thin. The erythema on the abdomen remained similar to that seen in April, while the skin lesions on the hips had disappeared.
Pruritis: None
Dyspepsia: His food intake had also increased. He was able to eat about 2/3 of a bowl of rice at a time, and his appetite had returned.
-
-
-
Research consent
Prior to publishing this case report, we explained the collection and utilization of medical information to the patient and obtained his consent for the use of photographs and information of his case.
Changes in psoriasis according to treatment duration
Changes of PASI, average of pruritis VAS and average of dyspepsia VAS
Psoriasis Area and Severity Index (PASI)
Pruritus and dyspepsia assessment using Visual Analog Scale (VAS) scores
Discussion
Studies of herbal medicines for the treatment of psoriasis have focused on their anti-inflammatory and suppressive effects on certain immune mediators, just as Western medications. In particular, the relationship between chronic low-grade inflammation and psoriasis continues to be studied, and herbs with anti-inflammatory properties have been reported. Herbs including Scutellaria baicalensis Georgi Radix (黃芩), Rehmannia glutinosa (Gaertner) Liboschitz Radix (地黃), Coptis japonica Makino Rhizoma (黃蓮), Paeonia lactiflora Pallas Radix Rubra (芍藥), and Taraxacum platycarpum H. Dahlstedt Herba (蒲公 英) reportedly inhibit nuclear factor kappa-light-chain-enhancer of activated B cells (NF-κB) through various pathways and reduce the expression of various inflammatory mediators, including tumor necrosis factor-α, interleukin (IL), and chemokines. Persicaria tinctoria H. Gross Levis (靑黛) reportedly has an IL-17 inhibitory effect11). In addition, oxidative stress–related pathways, such as mitogen-activated protein kinase, NF-κB, and c-Jun N-terminal kinase, are directly associated with the pathology of psoriasis. This suggests that antioxidants such as Scutellaria baicalensis Georgi Radix (黃芩), Bupleurum falcatum Linne Radix (柴胡), and Phellodendron amurense Ruprecht Cortex (黃柏) may be used to treat psoriasis12). As described above, previous publications suggested the use of anti-inflammatory and antioxidant herbs to improve systemic inflammatory responses. However, steroids powerfully suppress inflammatory symptoms. Thus, it is less advantageous for Korean medicine to focus on the same as Western medicine via the study of anti-inflammatory and immune mediator suppressive actions7).
In other words, treating psoriasis with Herbal medicine should use a different perspective. Psoriasis is recognized as a systemic disease involving chronic inflammation of multiple organs, not just the skin. Metabolic syndrome and psoriasis can act as mutual risk factors, so it is recommended that glucose levels and blood pressure be managed in affected patients13). The study of lipid metabolism, particularly in psoriasis, has been ongoing since the early 20th century. Patients with psoriasis reportedly have abnormalities in blood lipid levels, skin barrier lipid structure, and receptors that transport lipids in the skin and blood. These findings suggest that lipid metabolism is involved in the pathology of psoriasis14).
Compared to healthy individuals, psoriasis patients have been reported to have significant increases in blood cholesterol, low-density lipoprotein cholesterol, and triglycerides, and a significant decrease in high-density lipoprotein cholesterol, which transports cholesterol deposited in the periphery to the liver. It has also been reported that plasma antioxidant markers, including glutathione, are reduced and lipolysis disorders with decreased bile juice concentration. Moreover, significant amounts of cholesterol are also detected in scales of psoriatic lesions. It is 12–23 times higher than healthy people who secrete 85mg of cholesterol. There is a correlation between the amount of lipids secreted into the skin and the moderate severity of psoriasis. It has been suggested that the excessive scaling seen in psoriatic skin may be a form of neutralizing cholesterol wastes19). Therefore, utilizing an herbal decoction to regulate lipid metabolism and digestive function may benefit patients by improving the condition of psoriatic skin lesions, managing metabolic syndrome, and reducing the side effects of concomitant Western medications7).
In addition to lipid metabolism, Leaky Gut Syndrome (LGS) can also be a pathologic factor of psoriasis. LGS is a disorder in which the intestinal mucosa is damaged. It leads to poor absorption of essential nutrients that should be absorbed normally. And absorption of substances that should not enter the body disrupt human immune system. Mucosal cells contain numerous microvilli and are held together by tight junctions. When the tight junctions between the microvilli and the intestinal mucosa cells are disrupted, LGS occurs. As mentioned earlier, patients with psoriasis often have lipid metabolism dysfunction and bile acid deficiency, resulting in high concentrations of endotoxins in the blood, and peptidoglycans from bacteria absorbed from the gut have direct toxic effects on the liver and skin15), which can lead to systemic inflammatory skin lesions such as psoriasis. Therefore, if endotoxins and wastes from the small intestine, large intestine, liver, and gallbladder are detoxified, both the digestive system and skin lesions may improve.
The patient in this case showed 92.6% improvement in PASI score after 2 months of treatment, demonstrating the successful effect of Jeongri-tang Gagam-bang (正理湯加減方) and acupuncture treatment. He had been taking medication for hyperlipidemia for 40 years. The long duration of psoriasis might be due to dysfunctional lipid metabolism. In Korean medicine, the lipids in the blood that are not being metabolized are classified as dampness (濕). Jeongri-tang Gagam-bang (正理湯加減方), a combination of Pyeongwi-san (平胃散), Hyangso-san (香蘇散) and Leejin-tang (二陳湯), consists of herbs that support digestive function and remove wastes, dampness (濕) from the digestive systems. Citrus aurantium L. Fructus Immaturus (枳實) improves skin barrier function directly through the peroxisome proliferator-activated receptor-β/γ7), and Hyangso-san (香蘇散), like Citrus aurantium L. Fructus Immaturus (枳實), regulates immune activity by increasing peroxisome proliferator-activated receptor-γ protein levels16). In addition, Pyeongwi-san (平胃散) reduced the amount of total cholesterol and triglycerides in animals with high-fat diet–induced obesity17). Changbakleejin-tang (蒼朴二陳湯), which is included in Jeongri-tang Gagam-bang (正理湯加減 方), had a significant effect on reducing total cholesterol, triglycerides, and β-lipoprotein content18).
Furthermore, the Sagwan(四關) point, composed of LI4 (合谷) and LR3 (太衝), is a very important treatment for almost all gastrointestinal disorders such as digestive disorders and abdominal bloating. Animal studies have shown that the Sagwan (四關) point has no effect on gastrointestinal motility in healthy conditions but normalizes the gastrointestinal system in pathological conditions in which gastrointestinal motility is overexcited or inhibited19). Acupuncture on the CV12 (中脘) and ST25 (天樞) points modulates inflammation and promotes fat metabolism in rats with high-fat diet–induced obesity20). The weekly acupuncture treatments, along with the daily Jeongri-tang Gagam-bang (正 理湯加減方), may have helped improve the digestive function of our patients with psoriasis.
Despite the fact that Jeongri-tang (正理湯) is composed of commonly used herbal medicines in Korea insurance system, there are no case reports of Jeongri-tang being used for skin diseases. Therefore, this study is significant in that it clinically confirmed the ability of Jeongri-tang Gagam-bang (正理湯加減方) to treat skin diseases by improve digestive system function. In addition, since the patient’s symptoms were significantly improved after Jeongri-tang Gagam-bang (正理湯 加減方) administration, we believe that it can be actively utilized in the future treatment of psoriasis. However, since this was a single case report, it is difficult to generalize the diagnostic method used herein. Thus, further studies are needed to expand the clinical usefulness of Jeongri-tang Gagam-bang (正理湯加減方) administration.
Conclusions
An 82-year-old man with psoriasis was successfully treated with Jeongri-tang Gagam-bang (正理湯加減方) twice daily for 90 days and once-weekly acupuncture treatment on the following acupoints for 15 min: CV12 (中脘), ST25 (天樞), GV20 (百會), LI4 (合谷), and LR3 (太衝). The following results were observed:
The patient had been taking medication for hyperlipidemia, type 2 diabetes, and hypertension for 40 years and had been treated for psoriasis for 20 years. One month before the start of treatment, his psoriasis worsened and the symptoms of dyspepsia and anorexia occurred, so he started Oriental medicine treatment.
Before treatment, erythematous plaques with overlying silvery scales were scattered across the arms, legs, abdomen, and hips (PASI – 21.6). Severe pruritus occurred on the limbs at night.
The patient was treated with Jeongri-tang Gagam-bang (正理湯加減方) twice daily for 90 days. A 1-month course of Jeongri-tang Gagam-bang (正理湯加減方) led to 74.1% improvement of the cutaneous lesions (to a PASI of 5.6) compared to his first visit. The pruritus and indigestion also improved.
A 2-month course of Jeongri-tang Gagam-bang (正理湯加減方) led to almost complete skin clearance and a 92.6% improvement in PASI (to 1.6) compared to his first visit. The pruritus, indigestion, and appetite also improved.
No adverse effects were reported.
Acknowledgement
This research was supported by Basic Science Research Program through the National Research Foundation of Korea (NRF), funded by the Ministry of Education under grant [No. NRF-2021R1I1A3A04037158].