Qualitative study on the key elements of obesity counseling in Korean Medicine
Article information

Abstract
Objectives
Weight counseling is an inevitable process for patients with obesity who intend to lose weight; however, the contents of real-world counseling practices remain uncertain in Korean medicine (KM) practice. This study aimed to explore the structure and constituents of obesity counseling in KM.
Methods
Qualitative methods were used to explore the structure of weight counseling and clinicians' approaches to weight counseling, particularly the advice and main constituents of weight counseling in KM. Nine KM clinicians (4 women, 5 men) from nine clinics completed face-to-face, individual and semi-structured interviews from September 2019 to February 2020 in Seoul, Daejeon, Cheonan, Seongnam, Asan, and Hwaseoug. The interviews were digitally recorded, transcribed verbatim, and categorized based on their constituents.
Results
During weight loss counseling, the six principal constituents of KM identified were: planning with patients, motivation, correcting misinformation on weight loss, dietary and exercise advice, medication guidance, and customized guides for each type.
Conclusion
Clinicians with in-depth knowledge about obesity prescribed personalized guidance for exercise, diet, and medication through an integrative approach. The study results provide an in-depth understanding of weight counseling in KM. These six constituents could guide the counseling provided by clinicians in obesity care.
Introduction
Obesity prevalence has increased worldwide in the past 50 years, with over one-third of the world's population now classified as obese1,2). The number of people with a body mass index (BMI) of >30 kg/m2 is expected to increase from 3.5% in 2005 to 9.0% in 2030 in South Korea3). The socioeconomic loss due to obesity amounted to 7.5 billion USD in 2015, which has doubled in the last 10 years in South Korea3).
The first-line treatment for obesity includes lifestyle interventions such as diet, physical activity, and behavior therapy. Medication and bariatric surgery are considered secondary therapeutic options4). To date, obesity treatment strategies have been unsuccessful in the long term 2). Only approximately 15% of patients with obesity experience weight loss; however, one-third return to their initial weight, while most fail after 5 years5). However, sustainable weight loss may be achieved with adequate clinician guidance through counseling. Hence, obesity requires comprehensive and multicomponent approaches, including lifestyle or behavioral training, dietary changes to reduce energy intake, and an increase in physical activity.
Counseling includes comprehensive education, lifestyle advice, and psychological support6). It is a major way to stabilize patients’ psychological urges to overeat, correct their weight loss knowledge, and eventually balance their energy input and output. Several guidelines have been developed to assist clinicians in promoting effective counseling7,8). These guidelines cover various fields ranging from counseling purposes to behavioral strategies. Clinicians use these guidelines to outline obesity counseling strategies 6).
Previous studies have used qualitative methods to explore clinicians’ approaches to weight management counseling, including the advice provided during routine consultation9–14). However, previous studies' interviewees have been limited to primary clinicians or general practitioners working in community health centers. They focused on how doctors raise obesity issues among patients who present to their clinics for other medical reasons. Thus, counseling for weight loss is easily overlooked, and doctors tend to be negatively disposed to it10–12,14).
In South Korea, there are many specialized obesity Korean Medicine (KM) clinics that mainly focus on obesity management. The number of such clinics has rapidly increased, with more than 3,000 clinics in Seoul, the capital of South Korea, alone15,16). This popularity is due to the success of clinicians meeting the needs of patients who want personalized weight loss treatment specific to their physical state while minimizing adverse effects17). In addition, a manual for standard counseling of patients with obesity in KM was developed by recognizing counseling as an important factor in obesity management8). Patients with obesity go to specialized obesity KM clinics to manage their weight and not for other issues. Therefore, counseling should focus on advice for weight management rather than how a weight issue is brought up. However, there is currently no data on weight loss counseling practices in KM. Therefore, this study aimed to explore the structure and constituents of obesity counseling in KM using qualitative methods, which can describe the complexities of weight counseling, which typically cannot be captured through closed-ended surveys.
Methods
1. Study design
This prospective, qualitative study was conducted at KM clinics in Seoul, Daejeon, Cheonan, Seongnam, Asan, and Hwaseoug. This research was conducted in accordance with the Declaration of Helsinki. reviewed and approved by the Human Research Ethics Committee of the Korea Institute of Oriental Medicine (I-1908/006-001, 5 September 2019) for studies involving humans. Informed consent was obtained from all subjects involved in the study. Written informed consent has been obtained from the participants to publish this paper.
2. Study sample and recruitment
Nine clinicians were recruited from the Society of Korean Medicine for Obesity Research (https://obesity.or.kr/) to participate in face-to-face, individual, and semi-structured interviews. The SKMOR has more than 500 KM clinicians who have worked in specialized obesity clinics. Eligible clinicians were recruited by email using purposive18) and snowball sampling19). The clinicians completed a 4- or 6-year course in a nationally accredited KM university, had a KM doctor license certified by the Ministry of Health and Welfare in South Korea, and had more than 1 year of experience in medical management for weight loss.
3. Interviews and measure
The selected clinicians participated in face-to-face, individual, and semi-structured interviews. The interviews were digitally recorded and lasted for less than 1 h. The interview guide was developed by two of the authors who had worked as clinicians in specialized obesity KM clinics and were experts in qualitative methods. The interviews involved asking clinicians to describe their weight loss counseling experiences; the objectives and roles of counseling in obesity management; their advice for weight loss during counseling; what they say to their patients about their weight; the difference between KM clinicians and other experts, such as dietitians or personal trainers; counseling on obesity; and the customized strategies provided to patients during counseling. The clinicians also provided demographic information. They received a $100 gift card incentive for participating in this study.
4. Analysis
Audio recordings of the interviews were de-identified and transcribed verbatim. Two researchers read all the transcripts, determined the meaning of the units from each interview, marked each deviation in meaning by using a keyword related to the units, and organized each interview based on the meaning of the units that yielded a sketch of the preliminary constituents. One of these researchers is an expert in qualitative research, and the other is also an expert in qualitative research and served as the president in the Academy of Qualitative research for the past 5 years. Thereafter, the researchers prepared condensed descriptions of the units and read them to synthesize their constituents and identify the essential meaning of the descriptions20,21). Disagreements were resolved by discussion. The findings were validated by sampling representative responses from the entire team.
Results
1. Demographics
Table 1 lists the participants in this study. All were KM clinicians who treated and counseled patients with obesity. Years of practicing medicine in specialized obesity KM clinics ranged from 1 to 10 years.
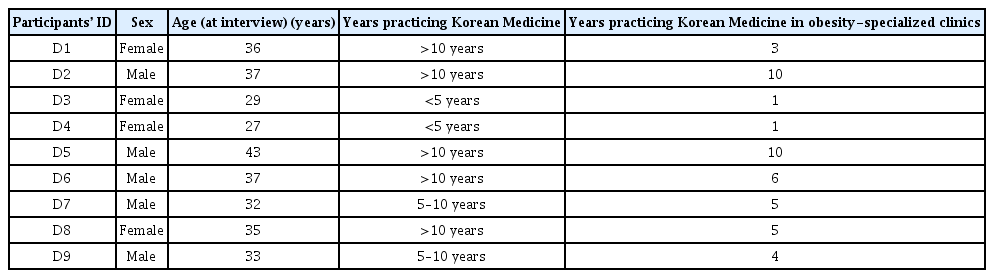
Participant Demographics
2. The structure of obesity counseling
The six constituents of obesity counseling in KM identified were planning with patients, motivation, correcting misinformation on weight loss, dietary and exercise advice, medication guidance, and customized guides for each type (Fig. 1).
Structure of obesity counseling in Korean medicine
1) Planning with patients
Setting goals and explaining prognosis
Clinicians set the final and monthly goals for individual patients. If patients tried to lose weight recently, they adjusted their goals according to their status (Table 2; quote 1). The clinicians explained the prognosis, especially the changes in body composition. Changes in body composition started with fat loss followed by muscle loss (Table 2; quotes 2 and 3).
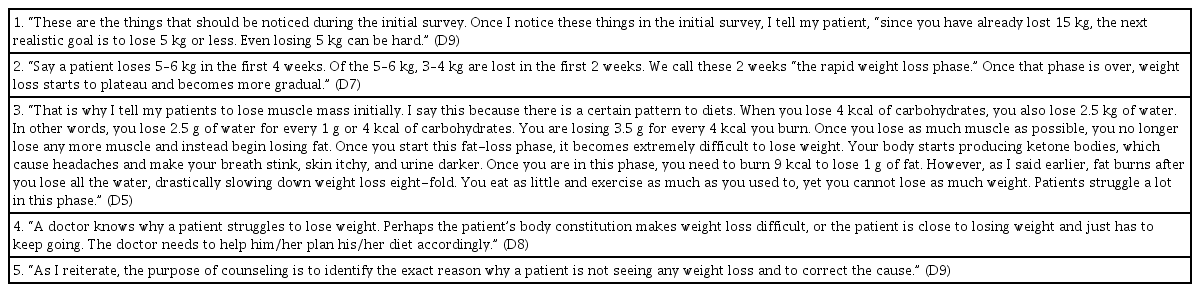
Quotations about Planning With Patients
Identifying the cause of slow weight loss
One of the clinicians’ roles was to identify the cause of slow weight loss, define it, and correct the cause (Table 2, quotes 4 and 5).
2) Motivation
Compliment and emotional support
Clinicians saw weight gain as a response to chronic stress. Therefore, it is necessary to reward patients to handle this stress. Dieting can also be stressful; however, achieving weight loss and being acknowledged for it are the first rewards that patients can give themselves. Clinicians emphasized that counseling for weight loss required encouragement or emotional support. They complimented the patients on their progress and told them to keep it up (Table 3; quote 1). Patients with obesity tend to have low self-esteem and negative thinking loops. Counseling is used to change patients’ perspectives (Table 3, quote 2).

Quotations about Motivation
Weight loss determination (initial examination)
An important factor in losing weight is to have patients complete their goals. Clinicians asked patients if their decision for weight loss was determined sincerely and made them commit to losing weight (Table 3, quote 3).
Monitoring
Clinicians played the role of a supervising figure (Table 3, quote 4). Patients were more apt to regulate their eating behavior while meeting with clinicians.
3) Correction of misinformation
Misinformation on diet
Controlling diet is mandatory for weight loss. Clinicians corrected the misinformation among patients who visited hoping for miracle medicine without diet control and asked them to count what they eat (Table 4, quotes 1, 2, and 3).
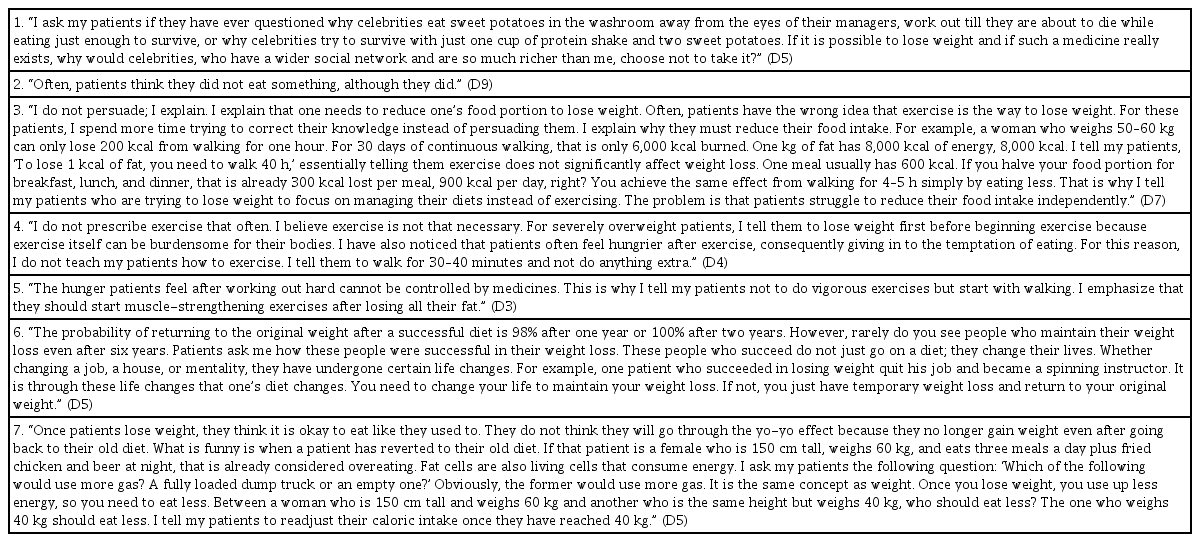
Quotations about Correcting Misinformation
Misinformation on exercise
Most patients have a misbelief that one must exercise to lose weight. However, excessive exercise causes patients to feel severely hungry and eat more. Eventually, excessive exercise is harmful to weight loss (Table 4, quotes 4 and 5).
Misinformation on weight maintenance
The participating clinicians agreed that weight loss is a lifelong journey, so patients should modify their lifestyle to maintain their weight (Table 5, Quote 6). In particular, eating habits and the reduction in the amount of food they consume should be maintained even if they succeed in losing weight (Table 4, quote 7).
Quotations about Diet and Exercise Advice
4) Diet and exercise advice
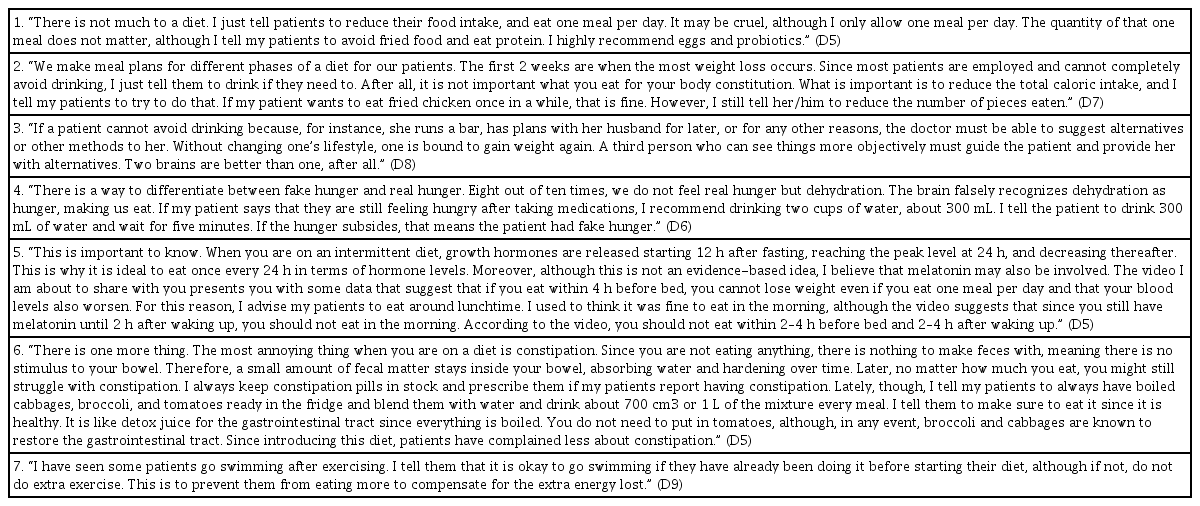
Limiting the amount of food/suggesting alternative/intermittent fasting
The clinicians advised the patients to reduce the amount of food they consumed. Some clinicians handed out menus (Table 5, quotes 1 and 2). Alternatives were provided if patients kept eating certain foods (Table 5, quotes 3 and 4). One clinician emphasized the importance of intermittent fasting (Table 5; quote 5). As patients are more prone to constipation in the diet process because they eat less, clinicians provided special recipes for constipation (Table 6, quote 6).
Quotations about Medication Guidance
Exercise guidance
The contents of exercise guidance are similar to those of exercise misinformation. The warned their patients against excessive exercise to avoid an increased appetite (Table 5, quote 7).
5) Medication guidance
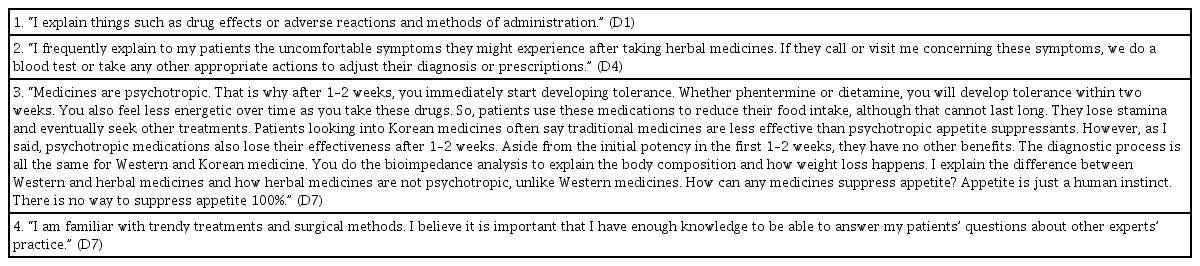
Medication guidance
It is obligatory for clinicians who prescribed medicine to give proper intake instructions and explain possible adverse reactions to the patients (Table 6; quotes 1 and 2).
Comparison with other treatments
Since there are various experts in obesity treatment, clinicians explain their treatment by comparing it with other treatments and give correct answers about efficacy, safety, and possible adverse effects of other treatments to patients (Table 6; quotes 3 and 4).
6) Customized guides for each type
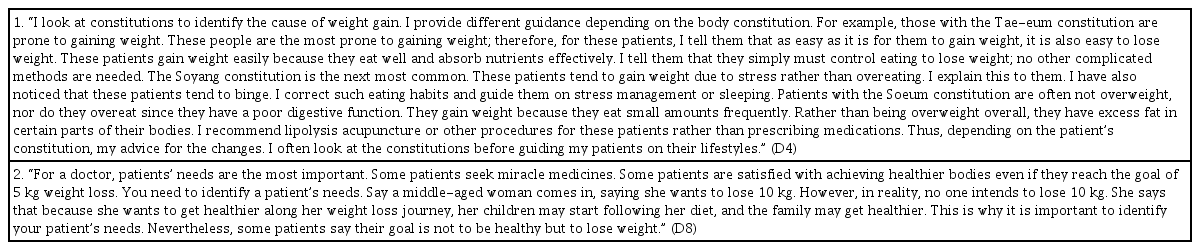
Constitution
Some clinicians used the patients’ Sasang constitution to identify the cause of weight gain and advise their lifestyle according to the constitution (Table 7, quote 1).
Quotations about Customized Guides for Each Type
Needs
The clinicians paid attention to the patient's words, situation, and environment, identified their needs, and set appropriate goals (Table 7, quote 2).
Discussion
This study is the first to qualitatively elicit the structure and constituents of obesity counseling in KM. A qualitative study method can provide broad and rich information and straightforward descriptions of clinicians’ perspectives on counseling for weight loss. This approach was useful in exploring the essential structure of weight counseling in KM22). An important finding of this study is that obesity counseling in KM is categorized into six constituents: planning with patients, motivation, correcting misinformation on weight loss, dietary and exercise advice, medication guidance, and customized guides for each type. A previous study included chart reviews on counseling for weight loss in KM in 2020; however, the chart had insufficient data and focused only on evaluating the patients’ condition and habits23).
Our findings suggest that the role of KM clinicians extends beyond prescribing medicine and covers the roles of dietitians and exercise therapists. Kushner et al. insisted that all patients should be counseled regarding evidence-based lifestyle approaches encompassing diet, physical activity, and behavioral change therapies as a foundation24). While weight counseling in KM follows a simple rationale, namely reducing energy intake and increasing physical activity, clinicians with in-depth knowledge about obesity prescribe personalized guidelines encompassing exercise, diet, and medications through an integrative approach25). Accordingly, KM clinicians conduct this work themselves rather than referring patients to nutritionists or dietitians.
Since weight loss primarily depends on reducing total caloric intake24), the correction of misinformation is mainly focused on reducing caloric intake. Thus, explaining the reasons for reducing caloric intake was emphasized based on recent research; for example, one technique for calorie reduction is intermittent fasting, which requires periods of voluntary abstinence from food and drink26,27). The lack of correction of misinformation is evident in a recent systematic review of weight control registries, where weight loss maintenance was mainly correlated not with exercise (planned, structured, and repetitive bodily movement done to improve or maintain one or more components of physical fitness), but with physical activity (any bodily movement that increases energy expenditure; e.g., activities of daily living like walking, climbing stairs, gardening, and others) and total energy intake24,28). Conversely, the difference between KM clinicians and other experts lies in understanding the patient's situation and finding alternative meal replacements, instead of forcing them to cut calories. Clinicians helped their patients set realistic physical activity goals, such as walking for an hour rather than jogging29).
Some clinicians used the Sasang constitutional theory to categorize patients with obesity and advise their lifestyle according to their type30). Sasang constitutional medicine is a tailored KM that classifies patients into four types: Taeyang, Soyang, Tae-eum, and Soeum. Each constitution is classified by characteristics of body shape, face, voice, and psychological and physiological aspects. A previous cross-sectional study on 3,348 subjects revealed the prevalence of obesity varies according to Sasang constitution; particularly Tae-eum was highly associated with an increased odds ratio for abdominal obesity. Thus far, the Sasang constitution has been considered a risk factor in predicting obesity30).
Establishing reasonable goals is important in obesity care. Patients with obesity often desire to achieve ideal weight; however, setting and accepting a modest weight loss goal is critical to prevent future disappointment and maintain motivation; thus, clinicians should view treatment for obesity as a lifelong process29). Clinicians should make patients aware of the need for continuous weight maintenance efforts, even after initial successful weight loss. Many factors, including environment, physiology, and behavior, may contribute to weight maintenance, much like the saying, “you need to change your life if you want to maintain weight.” Specifically, these changes involve regular breakfast intake, increased consumption of vegetables and fiber-rich foods, limited intake of certain types of foods such as fatty and sugary foods, consumption of healthy foods and few high-fat foods available at home, and having regular meal frequency according to weight control registries28).
Interestingly, the counseling was based on compliments and emotional support. This mirrors the research of Serdula et al.29); the more physicians counsel with an empathetic attitude and recognize the challenges and frustrations involved in trying to lose weight, the more likely the patient will feel supported and understood. Commitment to weight loss is similar to 5A, which asks about the patient’s readiness to lose weight, in the management algorithm for obesity in primary care31). This indicates that clinicians should determine if patients are motivated to lose weight and assess patients’ willingness to invest substantial time, effort, and expenses required for weight loss treatment. Frequent monitoring is important, as a significant association between monitoring and weight loss was consistently found in a systematic review32). Continuous monitoring by clinicians also facilitates communication with patients.
Patients with obesity have plenty of accessible information and seek a healthy and effective way to lose weight. Interestingly, one of the least frequently reported strategies from people who succeeded in weight loss was information seeking (seeking weight loss information online)28). Therefore, clinicians should be aware of the possible treatment options and provide accurate information about treatments, efficacy, safety, and possible adverse effects. In addition, all clinicians should be educated to provide standardized and effective counseling using a manual8). A previous chart review reported diverse counseling quality and content among KM clinicians. The lack of specific guidance in obesity counseling could be improved through education and dissemination of the manual23).
This study had some limitations. Because of the nature of qualitative research, the findings cannot be extrapolated to all clinicians and should be considered with regard to the generalizability of findings.
In conclusion, counseling for weight loss in KM encompasses a variety of themes, including diet, exercise, motivation, goal setting, and advice for each patient type. Clinicians with in-depth knowledge about obesity should prescribe personalized guidelines encompassing exercise, diet, and medication through an integrative approach. This study provides an in-depth understanding of obesity counseling in KM. The constituents could guide clinicians' counseling in obesity care. Future studies should investigate the efficacy of counseling in clinical trials.
Acknowledgments
The authors would like to thank the participants of this study and the Society of Korean Medicine for Obesity Research.
Notes
Conflicts of Interest
The authors declare that they have no conflicts of interest.
Funding
This research was supported by the Association of Korean Medicine (ERN1911130), the Korea Institute of Oriental Medicine (KSN2022210), and the Korea Health Technology R&D Project through the Korea Health Industry Development Institute (HF20C0208). The funders have no role in the review, preparation of the manuscript, or decision to publish.
Data Availability Statement
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.