The Retrospective Study of Advanced Cancer Patients Receiving Integrative Cancer Treatments in single Comprehensive and Integrative Medicine Hospital
Article information

Abstract
Objectives
Traditional Korean medicine (TKM) has been supplied as part of a national health care system in South Korea under a dual medical system, however it has been difficult to mix western medicine and TKM medical practices in existing hospitals. For the objective of innovative integration between them. Comprehensive and Integrative Medicine Hospital were founded in Daegu, South Korea. Here, we discussed the clinical outcomes of cancer patients who received integrative cancer treatment (ICT).
Methods
A total of 678 patients previously diagnosed with cancer were retrospectively checked in our institution for 2 years. After applying inclusion/exclusion criteria, 573 patients were eligible for the final analysis. The overall survival (OS) of these patients in the aftercare period were determined. We looked at how clinical factors and treatments including chemotherapy, complementary and alternative medicine (CAM), and TKM affected the OS.
Results
At the first visit, 218 subjects had no evidence of disease after tumor resection and 355 ones with advanced cancer, who receiving ICT including chemotherapy, CAM, and TKM showed better OS compared to the CAM including TKM or the best supportive care (median OS = 216, 78, and 46 days, respectively). The median OS was not reached in TKM only, even though the sample size was small (N=12). Even after adjusting for clinical factors associated to liver, renal, and hematologic manifestation, ICT still remained significant.
Conclusions
We demonstrated that ICT might be beneficial for advanced cancer regardless of the performance status, liver and renal function, since it positively affected the OS.
Introduction
Along with the increase in the incidence of cancer patients, the frequency of use of complementary and alternative medicine (CAM), including traditional Korean medicine (TKM), has increased, which has been offered to many cancer patients in major developed countries including the United States1,2). In detail, National Center for Complementary and Integrative Health in the United States has established a strategy to develop CAM every five years. As a result of these efforts, the National Comprehensive Cancer Network (NCCN) recommended the use of acupuncture in 5 out of 11 guidelines for cancer treatment, and among 45 major cancer centers designated by the National Cancer Institute (NCI) 40 hospitals provide the information on “acupuncture and herbal medicine” treatment as an ICT, and actually provide acupuncture treatment services to cancer patients3, 4). Furthermore, since the 2010s, clinical practice guidelines for the treatment of lung cancer and breast cancer using TKM, have been developed and published as articles in high-impact journals, and are being used in a variety of ways in major hospitals5,6).
In South Korea, a dual medical system for western medicine (WM) and traditional Korean medicine (TKM) has been implemented, with TKM being given as part of a national health-care system7). However, in current hospitals, the integration between them has not been successful. For the objective of implementing a drastic change from traditional healthcare services by combining the medical practices of WM and TKM, Comprehensive and Integrative Medicine Hospital (CIMH) were founded in Daegu, South Korea. We have reported the cases showing the successful outcomes in CIMH8,9).
Here, we discussed the clinical outcomes of cancer patients who received integrative cancer treatment (ICT). In detail, we investigated how beneficial ICT is for advanced cancer patients even after the clinical variables related with liver, kidney, and hematologic manifestation were adjusted.
Patients and Methods
1. Patients
We including an oncologist reviewed retrospectively the total of 678 cancer patients who had visited from Sep. 2015 to Aug. 2017 and been treated at the CIMH based on electronic medical records (EMR) including medical or image reports in other hospital. After 105 patients not receiving any treatments at the CIMH were excluded, 573 patients remained for the analysis.
Demographic characteristics including sex, age, the previous medical history (cancer-related surgery, chemotherapy regimen, radiation treatments, etc.), Eastern Cooperative Oncology Group (ECOG) performance status, all the treatments provided in the CIMH, were obtained from EMR. We classified them into 2 groups at first visit: 1) no evidence of disease (NED) 2) advanced cancer who were divided according to the treatments chosen by the patients (ICT, CAM, TKM, and BSC). This study was approved by the Institutional Research Board of the CIMH (Daegu, South Korea) (IRB No. CR-18-135).
2. The definition of each treatment
The WM means the conventional chemotherapy regimens provided by the oncologist in CIMH. The CAM group received at least one of treatments as follows: thymosin alpha 110) (a peptide hormone that is endogenously produced by the thymus gland and potentiates T cell-mediated immune response), Viscum album11) (the preparations from the parasitic plant mistletoe), selenium supplements12) glutathione13) high-dose vitamin C injection14) and local-regional hyperthermia15). The TKM group received herbal decoctions, acupuncture, or moxibustion, all of which were prescribed or used by TKM doctors in CIMH. The best supportive care (BSC) group received only palliative care without any anticancer therapies such as WM including chemotherapy, CAM, and TKM mentioned above.
3. Outcome measures
The overall survival (OS) was defined as the time from the first day of any treatments to the time of death from any cause or the end of the study (Feb. 28, 2018), or time of loss to follow-up. We compared the OS of all subjects or advanced cancer patients treated with ICT (Chemotherapy + CAM + TKM), CAM + TKM, CAM only, TKM only, or BSC. Furthermore, it was analyzed after ECOG performance status and various clinical variables were adjusted.
4. Statistical Analysis
Demographic characteristics and clinical features between groups (ICT, CAM, TKM, and BSC) were compared using ANOVA or Chi-square tests, as appropriate. Survival curves were estimated using the Kaplan-Meier method and statistically compared by the log-rank test. A Cox proportional hazard model analysis of OS was used to assess potential predictors of survival. A p-value < 0.05 was considered statistically significant, and all analyses were performed using the R statistical software 4.03.
Results
1. Patient characteristics
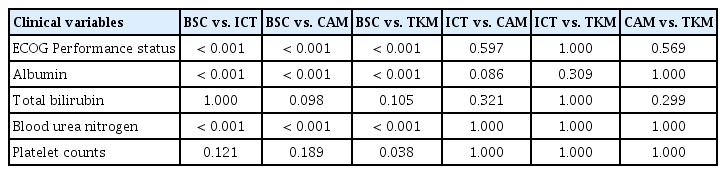
The main characteristics of our patient population are summarized in Table 1. Most of the patients were old (median age 60 years, range 10–91), with a low body mass index (median 21.6, range 12.5–40.9). The majority of cancer subtype was solid cancers such as breast (16.75%) and stomach (15.01%). In the NED group, the prognostic factors such as ECOG performance status and blood tests were significantly better compared to the advanced cancer group. The survival curve did not reach the median OS during the follow-up period (Figure 1A). Therefore, we excluded the NED group and focused on advanced cancer group. At first presentation, 206 patients (58.03%) had poor performance status (ECOG 3–4). The majority of them initially presented with general weakness and cancer pain. In detail, the BSC group showed considerably worse prognostic factors such as ECOG performance status, albumin, and BUN than the other treatment-specific groups (Table 1). The post-hoc analysis suggested that ICT, CAM, and TKM, on the other hand, had no discernible differences for the prognosis (Table 2).
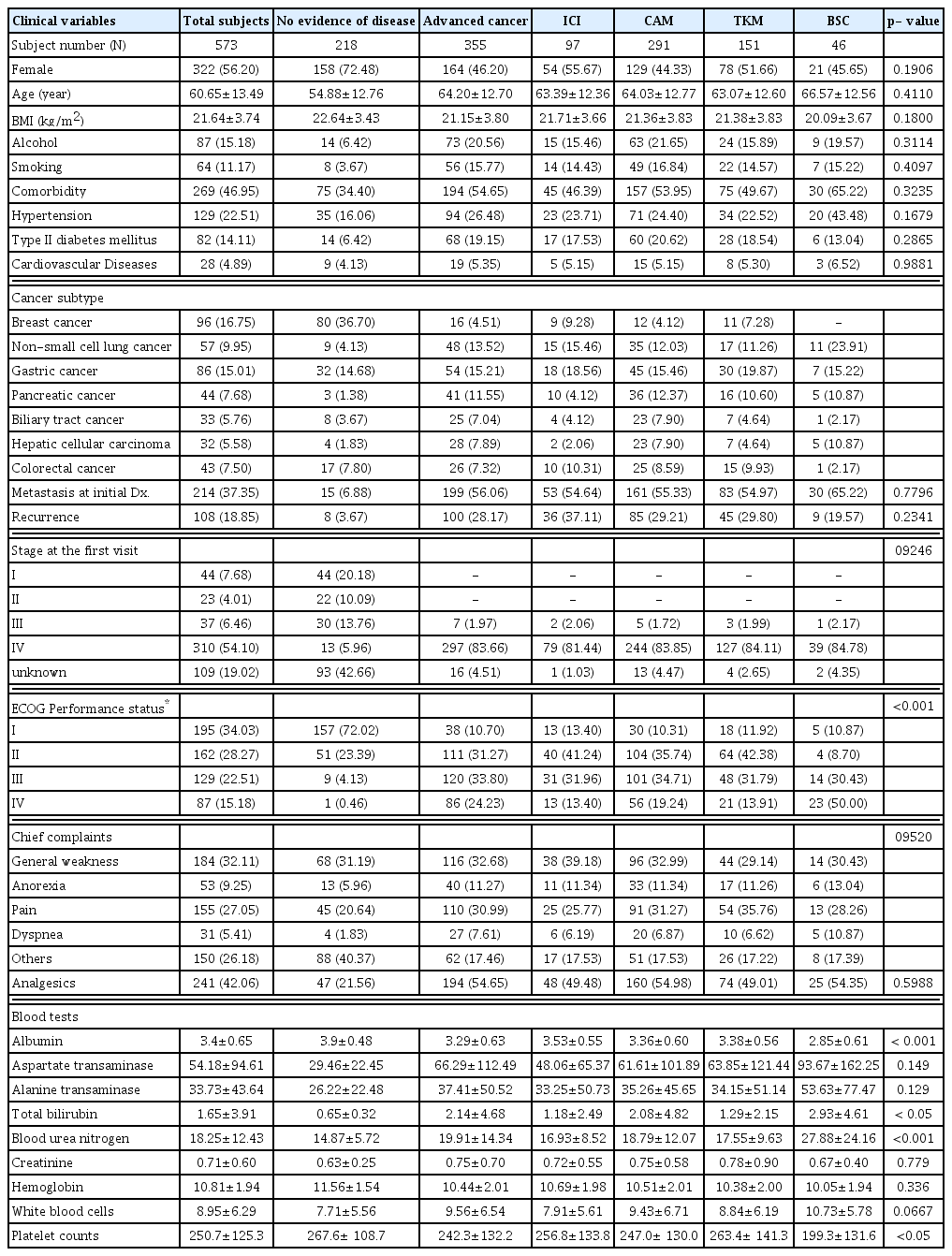
Demographic characteristics and clinical features of study subjects (N=573)
Kaplan-Meier survival plots for overall survival according to each group
(A) no evidence of disease (NED) vs. advanced cancer at first visit, (B) ECOG performance status: 1–4, (C) the combinations of treatments in the advanced cancer patients, (D) chemotherapy vs. no chemotherapy, (E) CAM vs. no CAM, and (F) TKM vs. no TKM. The p-values by the log-rank test were presented at the left bottom in each plot.
2. The outcomes based on overall survival
The median OS for the advanced cancer patients was 109 days [95% confidence interval (CI) 77–139] (Figure 1A). According to ECOG performance status, the survival curves were discretely separated (p < 0.001, Figure 1B). The type of treatment chosen by the patients is also a key in their prognosis (p < 0.001, Figure 1C). The patients receiving ICT including chemotherapy, CAM, and TKM showed better OS compared to the CAM and TKM or the BSC treatment (median OS = 216, 78, and 46 days, respectively). Interestingly, the median OS was not reached in TKM only, but the sample size was small (N=12). When compared to each control, chemotherapy and TKM showed statistically different OS (p < 0.001, Figure 1D & 1F), while the CAM did not (p = 0.09, Figure 1E).
By the univariate analyses, the significant prognostic factors were identified, and the performance status, analgesics intake, albumin, AST, white blood cells and the ICT in multivariate analyses were significantly independent prognostic factors for OS (Table 3).
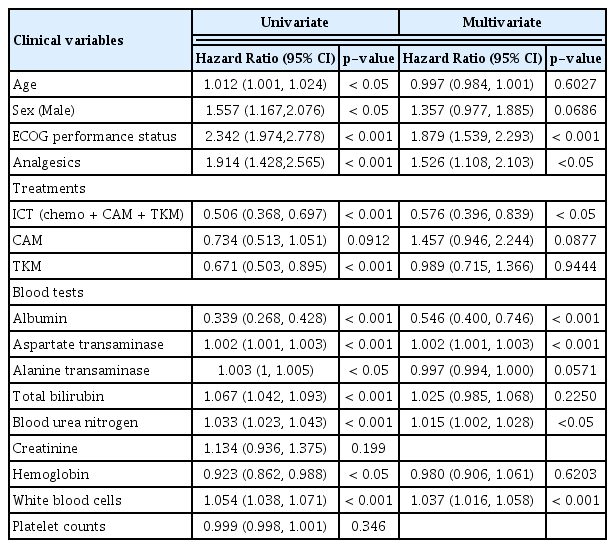
Univariate and multivariate analyses of clinical factors potentially associated with survival outcome
Discussions
TKM is being given to a large number of patients in South Korea in addition to WM. According to the findings of a TKM consumption survey conducted in Korea in the 2010s3) 74.4 percent of women use TKM, compared to 63.4 percent of men. Also, TKM was used 86.2 percent of the time by individuals in their 60s and above, compared to 39.0 percent by those under 30, suggesting the elderly’s preference for tkm16). In addition, disease treatment accounts for approximately 89.9% of the reasons for utilizing TKM. However, because the majority of illness are limited to musculoskeletal disorders, it is critical to expand TKM to include oncology, as leading cancer institutes in the United States have done. Furthermore, the elderly’s preference for TKM, which has been consistently observed in previous surveys on the use of TKM, is important in understanding the various medical demands for the increase in the number of cancer patients in the elderly due to Korea’s aging population and the resulting rise in cancer incidence17). It is important to collect data in order to establish proof for the efficacy and safety of tkm18,19).
Despite a policy to enhance coverage for serious diseases including cancer under the national health insurance system, the majority of TKM are not covered in contrast to WM20). It makes TKM utilized by the cancer patients in end-stage for whom WM is unavailable. Patients with a poor prognosis, thus, were included in the group receiving TKM, resulting in a skewed evaluation, such as minimizing TKM’s effectiveness. We have implemented the innovative strategy for combining the medical practices of WM and TKM in CIMH since it was found. The benefit of ICT with OS, the most reliable measure of clinical benefit in general, was revealed in the retrospective analysis based on the records in CIMH. The previous clinical studies across the major cancers including breast, liver, lung, stomach and colon demonstrated the adjuvant effect of herbal medicine for WM in patients with solid cancers by reducing the adverse effect and enhancing OS21–26). In detail, single herbs (Astragali Radix, Scutellariae Radix, Fritillaria thunbergii, Oldenlandia diffusa, Saposhnikoviae Radix, Polyporus umbellatus, Trichosanthis Radix etc.) are shown to prolong OS in lung cancer, and high doses of herbal formulas (Gamisoyo-san, Jibaekjihwang-hwan, Pyeongwi-san, Kamikwibi-tang, etc.) were associated with better survival in colorectal cancer. Also, long-term herbal treatment significantly reduces the risk of recurrence and metastasis after tumor resection27,28). However, most of cancer patients in South Korea usually receive the ICT after advanced stage as shown in our study.
With the survival benefit of TKM only observed, the application of TKM to cancer patients early on might help them have a better prognosis. Even though the clinical characteristics were quite similar between TKM and CAM groups (Table 1), only TKM in contrast to CAM had a superior OS than the control group (Figure IE & IF). Furthermore, the multivariate analysis suggested that CAM use would be harmful for the OS (HR: 1.457, 95% CI: 0.946–2.244, p = 0.0877), which needs to be analyzed in detail later. Our study has several limitations. First, our study design, retrospective cohort study is often assumed to have more bias and confounding since the data collection was not planned ahead of time29). The proportions of CAM and TKM were chosen based on the patient’s preferences. However, we tried to adjust as many prognostic factors for OS as possible, including the blood tests and ECOG performance status. Second, each of these treatments (ICT, CAM, and TKM) includes a variety of the methods. However, they haven’t been fully examined because they are so diverse. Also, a variety of cancer subtypes were included for the analysis. Third, we could not have the group receiving only chemotherapy for comparison because all the patients in CIMH receiving CAM or TKM. Instead, the BSC group was used even though they had substantial poor prognosis.
In conclusion, we suggested that TKM could increase the OS of advanced cancer patients when used in conjunction with chemotherapy, and improve survival to some extent even when used alone compared to CAM. The clinical research on specific treatments in TKM for specific cancer types is needed in the future.
Acknowledgements
This work was supported by a grant from the Comprehensive and Integrative Medicine R&D project through Comprehensive and Integrative Medicine Institute, funded by the Ministry of Health & Welfare, Republic of Korea (Grant Number: 090-091-3000-3038-301-320-01).