References
1. Cheng A, Leung Y, Brodaty H. 2021;A systematic review of the associations, mediators and moderators of life satisfaction, positive affect and happiness in near-centenarians and centenarians. Aging & Mental Health :1–17.
https://doi.org/10.1080/13607863.2021.1891197
.
5. Cummings JL, Morstorf T, Zhong K. 2014;Alzheimer’s disease drug-development pipeline: few candidates, frequent failures. Alzheimer’s Research & Therapy 6(4):37.
https://doi.org/10.1186/alzrt269
.
6. Lee DW, Shin GJ, Lee WC. 1995;A Comparative Consideration of Treatment on Dementia in Oriental and Occidental Medicine. The Journal of Dong Guk Oriental Medicine 4:67–80.
7. Xu QQ, Shan CS, Wang Y, Shi YH, Zhang QH, Zheng GQ. 2018;Chinese Herbal Medicine for Vascular Dementia: A Systematic Review and Meta-Analysis of High-Quality Randomized Controlled Trials. Journal of Alzheimer’s disease: JAD 62(1):429–456.
https://doi.org/10.3233/JAD-170856
.
8. Huang Q, Luo D, Chen L, Liang FX, Chen R. 2019;Effectiveness of Acupuncture for Alzheimer’s Disease: An Updated Systematic Review and Meta-analysis. Current Medical Science 39(3):500–511.
https://doi.org/10.1007/s11596-019-2065-8
.
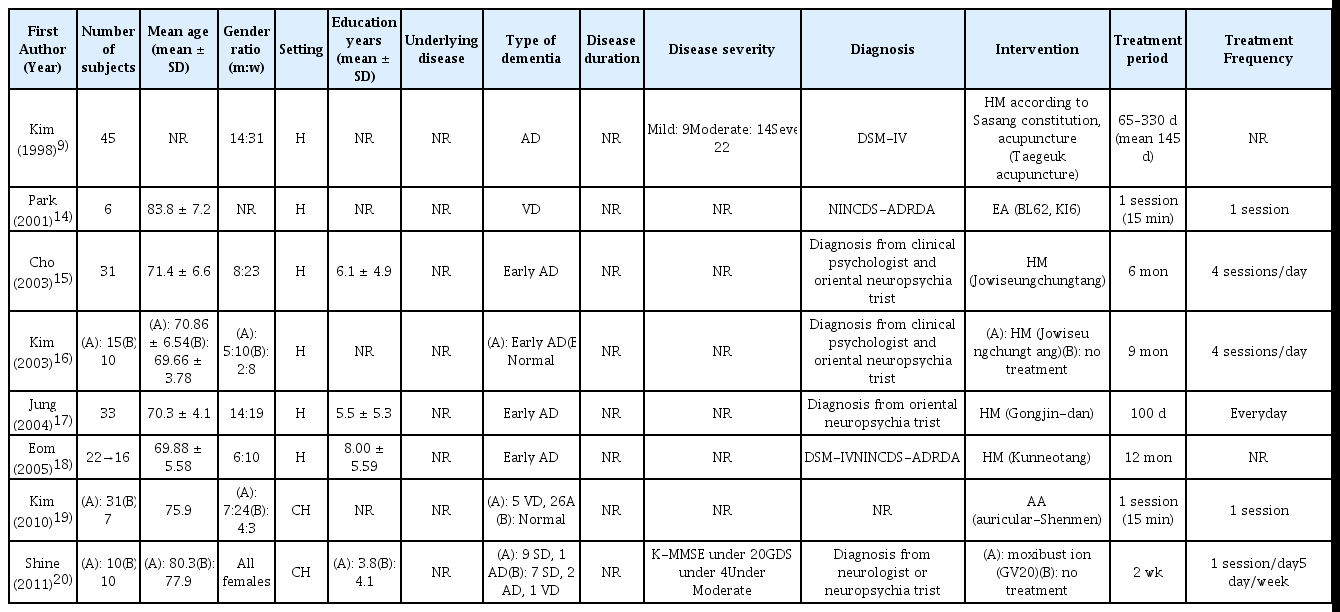
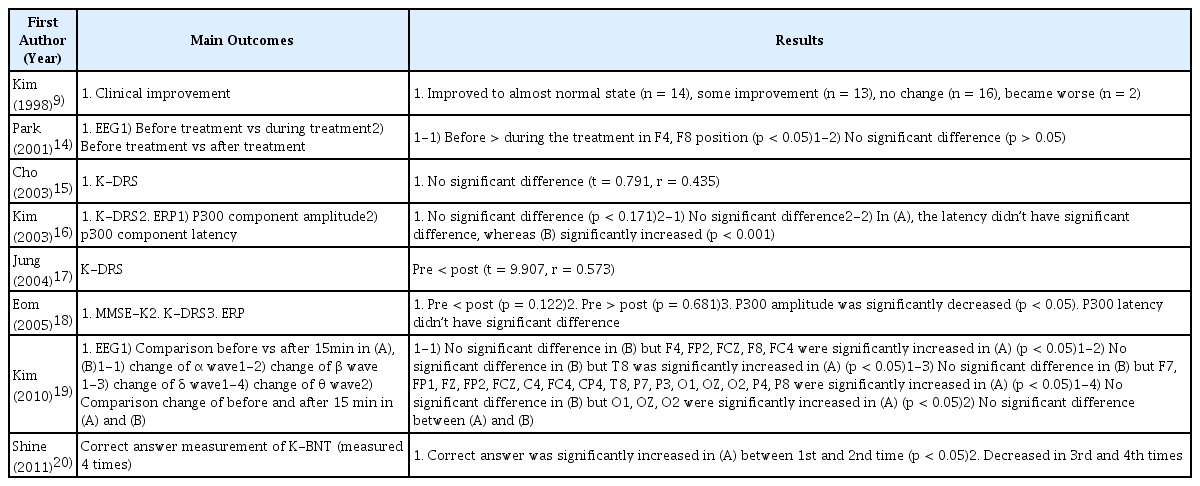
9. Kim BG, Hyun KC, Kim JW, Whang WW. 1998;A clinical study on the effects of oriental medical treatment on Dementia of Alzheimer type. J of Oriental Neuropsychiatry 9(1):25–43.
10. Bae DB, Park J, Lyu Y, Lee G, Jung H, Kang H, et al. 2012;The Case Report of 3 Dementia Patients Treated by Needle-Embedding Therapy. J of Oriental Neuropsychiatry 23(3):99–116.
http://dx.doi.org/10.7231/JON.2012.23.3.099
.
11. Ahn HI, Hyun MK. 2019;Effectiveness of integrative medicine program for dementia prevention on cognitive function and depression of elderly in a public health center. Integrative Medicine Research 8(2):133–137.
https://doi.org/10.1016/j.imr.2019.04.008
.
12. Higgins JPT, Thomas J, Chandler J, Cumpston M, Li T, Page MJ, et al. 2019. Cochrane Handbook for Systematic Reviews of Interventions John Wiley & Sons; Available from: URL:
https://handbook-5-1.cochrane.org/
.
13. Kim SY, Park JE, Lee YJ, Seo HJ, Sheen SS, Hahn S, et al. 2013;Testing a tool for assessing the risk of bias for nonrandomized studies showed moderate reliability and promising validity. Journal of Clinical Epidemiology 66(4):408–414.
https://doi.org/10.1016/j.jclinepi.2012.09.016
.
14. Park WS, Lee TY, Kim SY, Leem GG, Yuk SW, Lee CH, et al. 2001;The Immediate Effect of Electroacupuncture at the B62(Shinmaek) K6(Chohae) on the EEG of Vascular Dementia. The Journal of Korean Acupuncture & Mxibustion Society 18(2):67–78.
15. Cho S, Kim J, Kim H, Chung K, Whang W. 2003;A Study of Jowiseungchungtang in patients with mild Dementia of Alzheimer type. J of Oriental Neuropsychiatry 14(1):17–26.
16. Kim B, Kim J, Kim H, Chung K, Whang W. 2003;The effects on Jowiseungchungtang of patients with early DAT using auditory ERP and K-DRS. J of Oriental Neuropsychiatry 14(2):1–17.
17. Jung H, Jang H, Sung W, Lee S, Son J, Han S. 2004;A study of Gongjin-dan in patients with mild Dementia of Alzheimer type. J of Oriental Neuropsychiatry 15(2):141–148.
18. Eom HJ, Kim JW, Park E, Kim H, Whang WW. 2005;The Effects on Kunneotang of Patients with Early Dementia of Alzheimer Type -12 Months Clinical Study-. J of Oriental Neuropsychiatry 16(1):43–66.
19. Kim MR, Lee GE, Lee SE, Park IS, Park JH, No DJ, et al. 2010;The Effect of Auricular Acupuncture at the Shinmun on the Electroencephalogram(EEG) in patients with dementia. J of Oriental Neuropsychiatry 21(3):45–64.
20. Shine YJ, Choi YG, Jang WS. 2011;The Effect of Moxibustion Therapy on Dementia Patients ; Evaluated by K-BNT. The Journal of East-West Medicine 36(2):51–61.
21. Lee D. 2020;Analysis of Clinical Korean Medicine Studies on Dementia : Focused on Korean Literatures for 10 Years. Journal of Society of Preventive Korean Medicine 24(1):37–48.
https://doi.org/10.25153/spkom.2020.24.1.004
.
22. Takayama S, Tomita N, Arita R, Ono R, Kikuchi A, Ishii T. 2020;Kampo Medicine for Various Aging-Related Symptoms: A Review of Geriatric Syndrome. Frontiers in nutrition 7:86–86.
https://doi.org/10.3389/fnut.2020.00086
.
23. Ren ST, Wang L, Wu YR, Liu WW, Liu XJ, Wang YX, et al. 2018;Research Progress on Effective Ingredients of Traditional Chinese Medicine for Alzheimer’s Disease. Journal of Huaihai Institute of Technology, 27(3) :27–33.
https://doi.org/10.3969/j.issn.1672-6685.2018.03.007
.