References
1. Butler JV, Mulkerrin EC, O’Keeffe ST. Nocturnal leg cramps in older people. Postgrad Med J 2002;78(924):596–8.
2. Hallegraeff J, de Greef M, Krijnen W, van der Schans C. Criteria in diagnosing nocturnal leg cramps: a systematic review. BMC Fam Pract 2017;18(1):29.
3. Grandner MA, Winkelman JW. Nocturnal leg cramps: Prevalence and associations with demographics, sleep disturbance symptoms, medical conditions, and cardiometabolic risk factors. PLoS One 2017;12(6):e0178465.
4. Miller TM, Layzer RB. Muscle cramps. Muscle Nerve 2005;32(4):431–42.
5. El-Tawil S, Al Musa T, Valli H, Lunn MP, Brassington R, El-Tawil T, et al. Quinine for muscle cramps. Cochrane Database Syst Rev 2015;(4):CD005044.
6. Katzberg HD, Khan AH, So YT. Assessment: symptomatic treatment for muscle cramps (an evidence-based review): report of the therapeutics and technology assessment subcommittee of the American academy of neurology. Neurology 2010;74(8):691–6.
7. Man-Son-Hing M, Wells G, Lau A. Quinine for nocturnal leg cramps: a meta-analysis including unpublished data. J Gen Intern Med 1998;13(9):600–6.
8. Young G. Leg cramps. BMJ Clin Evid 2015;2015pii:1113.
9. El-Tawil S, Al Musa T, Valli H, Lunn MP, El-Tawil T, Weber M. Quinine for muscle cramps. Cochrane Database Syst Rev 2010;(12):CD005044.
10. Man-Son-Hing M, Wells G. Meta-analysis of efficacy of quinine for treatment of nocturnal leg cramps in elderly people. BMJ 1995;310(6971):13–7.
11. Young G. Leg cramps. BMJ Clin Evid 2009;2009pii:1113.
13. Blyton F, Chuter V, Walter KE, Burns J. Non-drug therapies for lower limb muscle cramps. Cochrane Database Syst Rev 2012;1:CD008496.
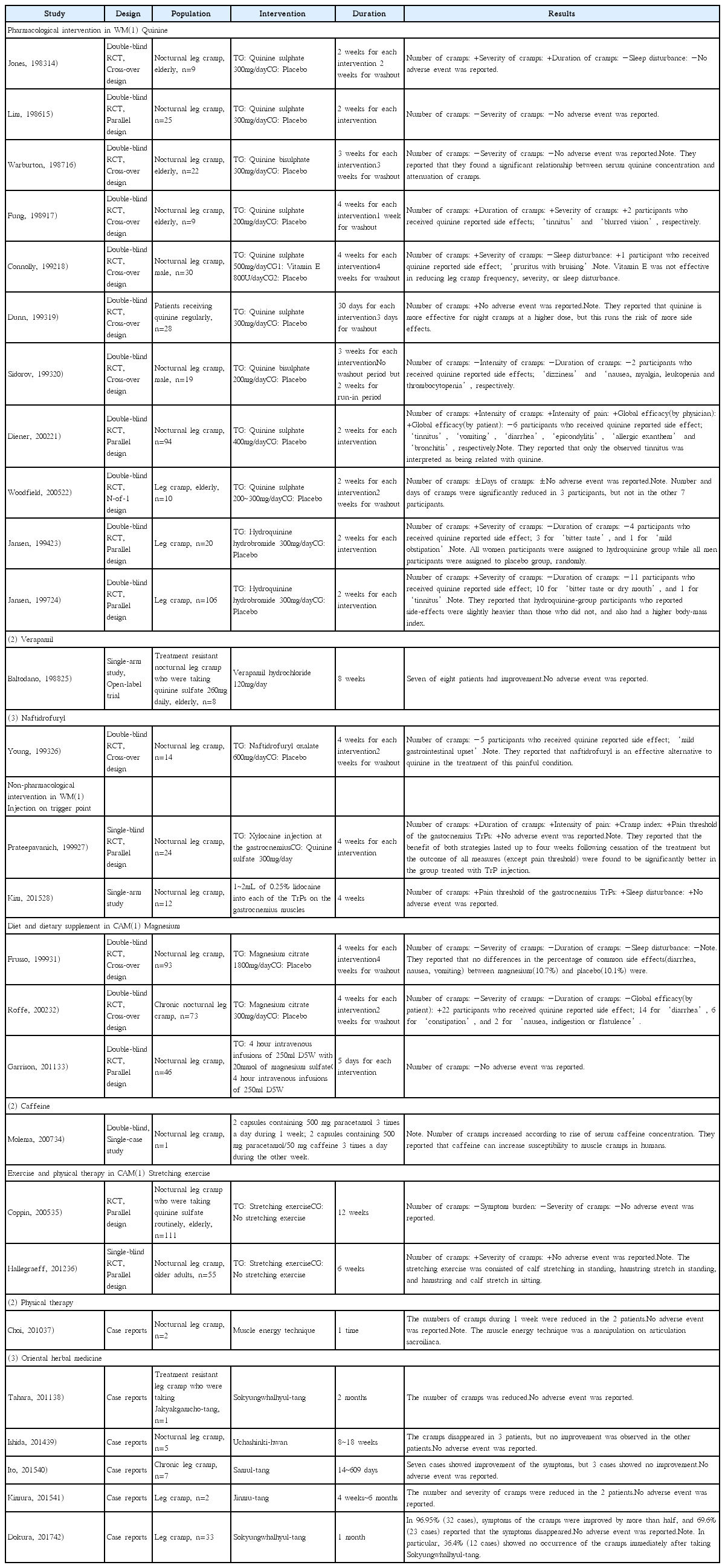
14. Jones K, Castleden CM. A double-blind comparison of quinine sulphate and placebo in muscle cramps. Age Ageing 1983;12(2):155–8.
15. Lim SH. Randomised double-blind trial of quinine sulphate for nocturnal leg cramp. Br J Clin Pract 1986;40(11):462.
16. Warburton A, Royston JP, O’Neill CJ, Nicholson PW, Jee RD, Denham MJ, et al. A quinine a day keeps the leg cramps away? Br J Clin Pharmacol 1987;23(4):459–65.
17. Fung MC, Holbrook JH. Placebo-controlled trial of quinine therapy for nocturnal leg cramps. West J Med 1989;151(1):42–4.
18. Connolly PS, Shirley EA, Wasson JH, Nierenberg DW. Treatment of nocturnal leg cramps. A crossover trial of quinine vs vitamin E. Arch Intern Med 1992;152(9):1877–80.
19. Dunn NR. Effectiveness of quinine for night cramps. Br J Gen Pract 1993;43(368):127–8.
20. Sidorov J. Quinine sulfate for leg cramps: does it work? J Am Geriatr Soc 1993;41(5):498–500.
21. Diener HC, Dethlefsen U, Dethlefsen-Gruber S, Verbeek P. Effectiveness of quinine in treating muscle cramps: a double-blind, placebo-controlled, parallel-group, multicentre trial. Int J Clin Pract 2002;56(4):243–6.
22. Woodfield R, Goodyear-Smith F, Arroll B. N-of-1 trials of quinine efficacy in skeletal muscle cramps of the leg. Br J Gen Pract 2005;55(512):181–5.
23. Jansen PH, Veenhuizen KC, Verbeek AL, Straatman H. Efficacy of hydroquinine in preventing frequent ordinary muscle cramp outlasts actual administration. J Neurol Sci 1994;122(2):157–61.
24. Jansen PH, Veenhuizen KC, Wesseling AI, de Boo T, Verbeek AL. Randomised controlled trial of hydroquinine in muscle cramps. Lancet 1997;349(9051):528–32.
25. Baltodano N, Gallo BV, Weidler DJ. Verapamil vs quinine in recumbent nocturnal leg cramps in the elderly. Arch Intern Med 1988;148(9):1969–70.
26. Young JB, Connolly MJ. Naftidrofuryl treatment for rest cramp. Postgrad Med J 1993;69(814):624–6.
27. Prateepavanich P, Kupniratsaikul V, Charoensak T. The relationship between myofascial trigger points of gastrocnemius muscle and nocturnal calf cramps. J Med Assoc Thai 1999;82(5):451–9.
28. Kim DH, Yoon DM, Yoon KB. The effects of myofascial trigger point injections on nocturnal calf cramps. J Am Board Fam Med 2015;28(1):21–7.
29. Garrison SR, Allan GM, Sekhon RK, Musini VM, Khan KM. Magnesium for skeletal muscle cramps. Cochrane Database Syst Rev 2012;(9):CD009402.
30. Sebo P, Cerutti B, Haller DM. Effect of magnesium therapy on nocturnal leg cramps: a systematic review of randomized controlled trials with meta-analysis using simulations. Fam Pract 2014;31(1):7–19.
31. Frusso R, Zárate M, Augustovski F, Rubinstein A. Magnesium for the treatment of nocturnal leg cramps: a crossover randomized trial. J Fam Pract 1999;48(11):868–71.
32. Roffe C, Sills S, Crome P, Jones P. Randomised, cross-over, placebo controlled trial of magnesium citrate in the treatment of chronic persistent leg cramps. Med Sci Monit 2002;8(5):CR326–30.
33. Garrison SR, Birmingham CL, Koehler BE, McCollom RA, Khan KM. The effect of magnesium infusion on rest cramps: randomized controlled trial. J Gerontol A Biol Sci Med Sci 2011;66(6):661–6.
34. Molema MM, Dekker MC, Voermans NC, van Engelen BG, Aarnoutse RE. Caffeine and muscle cramps: a stimulating connection. Am J Med 2007;120(8):e1–2.
35. Coppin RJ, Wicke DM, Little PS. Managing nocturnal leg cramps--calf-stretching exercises and cessation of quinine treatment: a factorial randomised controlled trial. Br J Gen Pract 2005;55(512):186–91.
36. Hallegraeff JM, van der Schans CP, de Ruiter R, de Greef MH. Stretching before sleep reduces the frequency and severity of nocturnal leg cramps in older adults: a randomised trial. J Physiother 2012;58(1):17–22.
37. Choi SH, Shin YI, Lee JY. Case Study; Manual Therapy for Patients with Calf Cramps. Korean J Orthop Manu Ther 2010;16(2):93–7.
38. Tahara E, Inutsuka H, Iwanaga J, Murai M, Ohtake M, Dokura J, et al. Four Patients with Calf Cramps who did not Respond to Shakuyakukanzoto but Responded well to Sokeikakketsuto. Kampo Med 2011;62(5):660–3.
39. Ishida K. Efficacy of Goshajinkigan in the Treatment of Sleep-Related Leg Cramps : a Study of Distinctive Patient Features from the Viewpoint of Kampo Medicine. Kampo Med 2014;65(2):100–7.
40. Ito T, Kimura Y, Ota S, Yamamoto S, Suda N, Nakazawa K. The Effectiveness of Shimotsuto Extract for Patients with Muscle Cramp. Kampo Med 2015;66(3):244–9.
41. Kimura Y, Sato H, Ito T. Three Cases of Calf Cramps with Internal Coldness Caused by Kidney Deficiency Presenting with Gastrointestinal Dysfunction Successfully Treated with Shimbuto. Kampo Med 2015;66(4):302–6.
42. Dokura J, Takahashi Y, Maeda H, Yoshinaga R, Inoue H, Yano H, et al. Review of 33 Patients in Whom Sokeikakketsuto was Used to Treat Recurrent Cramps of the Calf. Kampo Med 2017;68(1):40–6.
43. Nakae H. Treatment of Painful Muscle Cramp Due to Heat Injury Using Shakuyakukanzoto. Kampo Med 2013;64(3):177–83.
44. Wada K. Effect of Traditional Japanese Herbal (Kampo) Medicine, Goreisan, for Disdialysis and Muscle Cramps in Patients undergoing Maintenance Hemodialysis. Kampo Med 2012;63(3):168–75.
45. Manjra SI. Muscle cramps in athletes [thesis] St, Cape Town: University of Cape Town; 1991.
46. Lee JH, Lim JY. Muscle Cramps in Old Adults: Clinical Features and Pathophysiology. J Korean Geriatr Soc 2013;17(4):171–7.