Acupuncture as an adjunct treatment to increase the success rate of in vitro fertilisation: an overview of systematic reviews and meta-analyses
Article information
Abstract
Objectives:
To evaluate the effect of acupuncture as an adjunct treatment to increase the success rate of in vitro fertilisation (IVF).
Methods:
A review of the English and Korean literature was conducted to identify studies on acupuncture as an adjunct treatment to IVF. The main outcome measures were the biochemical pregnancy rate (BPR), the implantation rate (IR), the clinical pregnancy rate (CPR), the miscarriage rate (MR), the on-going pregnancy rate (OPR) and the live birth rate (LBR).
Results:
Nine meta-analyses of 11 systematic reviews (SRs) were included in this review. In four SRs, the overall IVF outcomes regardless of the procedural steps were documented; two of these SRs reported a significant effect on the CPR. One SR reported that acupuncture at the time of controlled ovarian hyperstimulation had a significant effect on the BPR. Seven SRs reported that acupuncture had no significant impact on transvaginal oocyte retrieval (TVOR). In eight SRs, significant impacts on the CPR, LIBR and OPR were reported when acupuncture was performed around the time of embryo transfer (ET). The results of repeated acupuncture after ET were included in two SRs, which included the same primary studies. The results of the SRs showed that acupuncture had a positive effect on the CPR.
Conclusions:
When the complete IVF procedure is analysed, there is conflicting evidence in that some reviews have found that acupuncture leads to an increased CPR but others have not. In addition, the reviews presented no evidence to suggest that acupuncture has any specific risks.
Introduction
Infertility is a common problem, affecting 717% of couples that desire children.1,2) In vitro fertilisation (IVF) is a costly treatment option for women, their partners and the public.3) Unfortunately, the average delivery rate for IVF per single initiated cycle using fresh, non-donor oocytes is still only 33%. Therefore, the majority of IVF cycles do not result in pregnancy, and typically multiple IVF cycles must be attempted to achieve pregnancy.4) There are no clear advantages of using adjunct therapies, which include medications (e.g., aspirin, glucocorticoids and growth hormone).5) Worldwide, the use of complementary and alternative medicine (CAM) therapies to overcome infertility has grown. Acupuncture is the most common form of CAM used for patients undergoing IVF.6)
Traditionally, the focus of acupuncture has been to restore the qi; however, there has been an increasing focus on acupuncture’s impact on neuromodulation and autonomic control.7) Because of the increased prevalence of acupuncture, the number of studies on this procedure has increased dramatically.8) The mechanism of acupuncture’s effectiveness in IVF is thought to involve the relief of emotional stress, an increase in blood flow to the pelvic cavity and the modulation of the functional control of the hypothalamic-pituitary-ovarian axis.3)
Randomised-controlled trials as well as several systematic reviews (SRs) and meta-analyses have examined whether acupuncture, as an adjunct to ART treatment, improves reproductive outcomes.10) There are many such reviews in the literature with conflicting findings. The aim of the present study was to critically analyse the findings in the literature.11,12)
Methods
Study Design
We used the methodology suggested by the Agency for Healthcare Research and Quality (AHRQ).13) Whitlock et al. introduced the concept of using previous SRs rather than creating a new SR when conducting comparative effectiveness reviews.14) Specifically, the effects of acupuncture at each IVF stage were examined separately.
Literature Search and Data Collection
The key question addressed in this study was the following: Does acupuncture increase pregnancy rates? A priori PICOTS-SD was predefined after consulting an Oriental medical gynaecologist who uses acupuncture. The PICOTS-SD was as follows:
Participants: Infertile women undergoing IVF
Interventions: Acupuncture as an adjunct treatment to IVF
Comparison: No restrictions
Outcome: No restrictions
Time: No restrictions
Setting: No restrictions
Study Design: Systematic reviews and meta-analyses
We searched PubMed and the Cochrane Library for relevant SRs published prior to 25 June 2012. We also reviewed the references of the relevant publications to identify any omitted publications.
Study Selection
The literature search and study selection were conducted independently by two reviewers (MKH and JCJ). Any disagreement regarding selection, extraction or quality was resolved by consensus or arbitration by an authoritative and experienced third reviewer (DIK). All SRs that evaluated the effect of acupuncture on women undergoing IVF were included. The language was restricted to English and Korean. All study designs other than SRs (i.e., narrative reviews, overviews and clinical guidelines) were excluded. Non-population-based and non-intervention-based reviews were also excluded.
According to the methods guide from the AHRQ, relevance should be evaluated to determine if an SR addresses the key questions being evaluated. We assessed the relevance of the selected SRs by predefined inclusion criteria and outcome measures.
Data Extraction and Quality Assessment
The data extraction form consisted of general SR information (i.e., title, year, authors and language), objective, searched databases, language restriction, inclusion and exclusion criteria, the number of included primary studies, the main results and the conclusions.
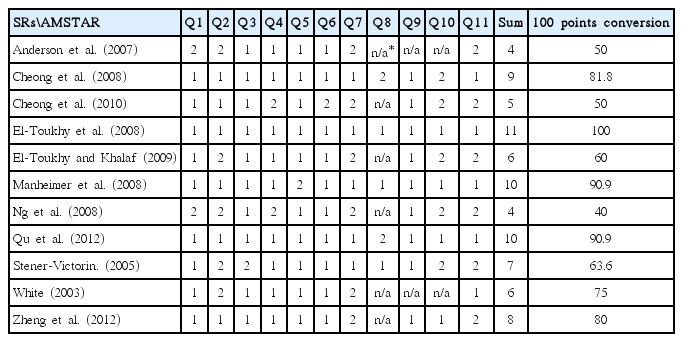
The methodological quality of the selected SRs was assessed using the assessment of multiple systematic reviews (AMSTAR) checklist. The AMSTAR checklist has good agreement, reliability, construct validity and feasibility and has been selected as the preferred instrument for assessing the quality of SRs by the World Health Organization and the Canadian Optimal Medication Prescribing and Utilization Service (COMPUS), among others.15) AMSTAR assesses 11 criteria for quality, and the choices are Yes, No, Cannot Answer and Not Applicable. The responses were graded as 1 for Yes, 2 for No, 3 for Cannot Answer and 4 for Not Applicable. The outcome of the quality assessment was allotted 1 point for Yes and 0 points for No and Cannot Answer. The aggregate total was calculated as the sum of the scores for each criterion, with a maximum of 11 points. If a non-applicable criterion existed, the highest point value was less than 11, and therefore, a 100-point conversion was created.
The data extraction and quality assessment were conducted independently by three reviewers (DJ, JCJ and JKP) with a predefined form. Any disagreement regarding selection, extraction and quality assessment was resolved by consensus or arbitration by an authoritative and experienced fourth reviewer (MKH and DIK).
Results
Selection of Primary SRs
A total of 95 studies were identified, including 29 studies from PubMed and 66 studies from the Cochrane Library. After eliminating ten duplicate articles, the titles and abstracts of the remaining articles were examined. Finally, the full text of 22 articles was reviewed. Eleven of the 22 articles were excluded because they were non-population based (n=8), non-intervention based (n=2) or included duplicate articles (n=1), which left 11 articles for the final analysis.11,12,16–24) Figure 1 shows the details of the selection process.
A Flowchart of the systematic review and meta-analysis selection process
Primary Studies Included in the SRs
The number of primary studies included in the SRs ranged from 3 to 24. The study that included the fewest primary sources was published in 2003 by White, who investigated infertility as a part of women’s reproductive health care. In 2012, Zheng et al. conducted a meta-analysis of 24 RCTs identified in July 2011. Unsurprisingly, larger numbers of primary studies were included in the more recent SRs. It should be noted that Cheong et al. (2008), Ng et al. (2008), Qu et al. (2012) and Zheng et al. (2012) searched Chinese databases and included primary studies conducted in China.
Quality of the SRs
The quality of the 11 selected systematic reviews was assessed using AMSTAR (Table 1). An a priori design was used in nine SRs, duplicate study selection and data extraction were conducted in six, a comprehensive literature search was performed in ten, and the status of the publication was used as an inclusion criterion in nine SRs. A list of included studies and the characteristics of the included studies was provided in ten SRs, and the scientific quality of the included studies was rated and documented in five SRs. In three of the five studies, the scientific quality of the included studies was used appropriately when formulating the conclusions. In nine SRs, the methods used to combine the study findings were appropriate. The likelihood of publication bias was assessed in four SRs, and conflicts of interest were stated in five SRs.
Quality of the Systematic Reviews
Previous standards were reviewed,13) and a consensus was reached that a score of 80 conversion points should be used as the cut-off for a good-quality study. Five reviews were above the cut-off score.
Total IVF Outcomes (Table 2)
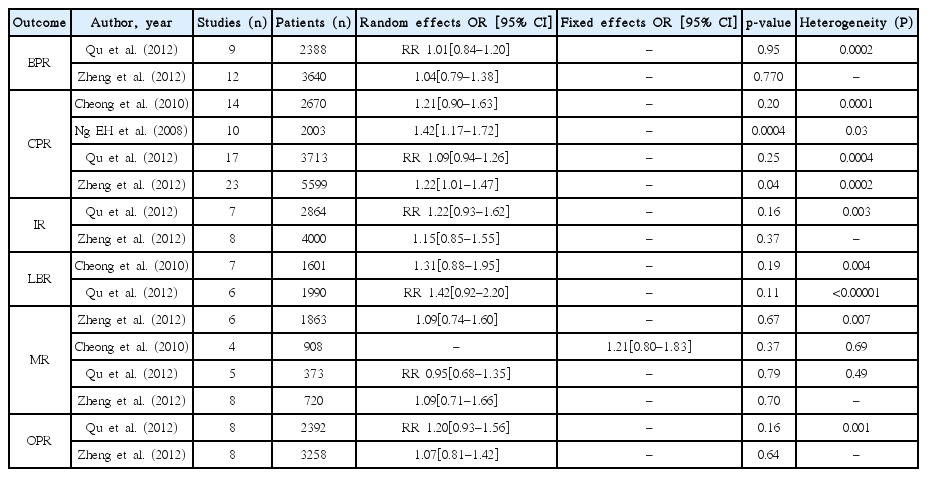
Main Outcomes of Meta-analyses in Total IVF Procedure
In four SRs, the total IVF outcomes regardless of the procedural steps were reported. Ng et al. (in 2008) and Zheng et al. in (2012) reported that acupuncture had a significant impact on the CPR (odds ratio (OR): 1.42; 95% confidence interval (CI): 1.17–1.72 and OR: 1.22; 95% CI: 1.01–1.47, respectively). Two reviews (Cheong, Qu) showed no effect on CPR. There were no significant differences in the BPR, IR, MR, OPR or LBR.
Outcomes of Acupuncture around COH and TVOR (Table 3)
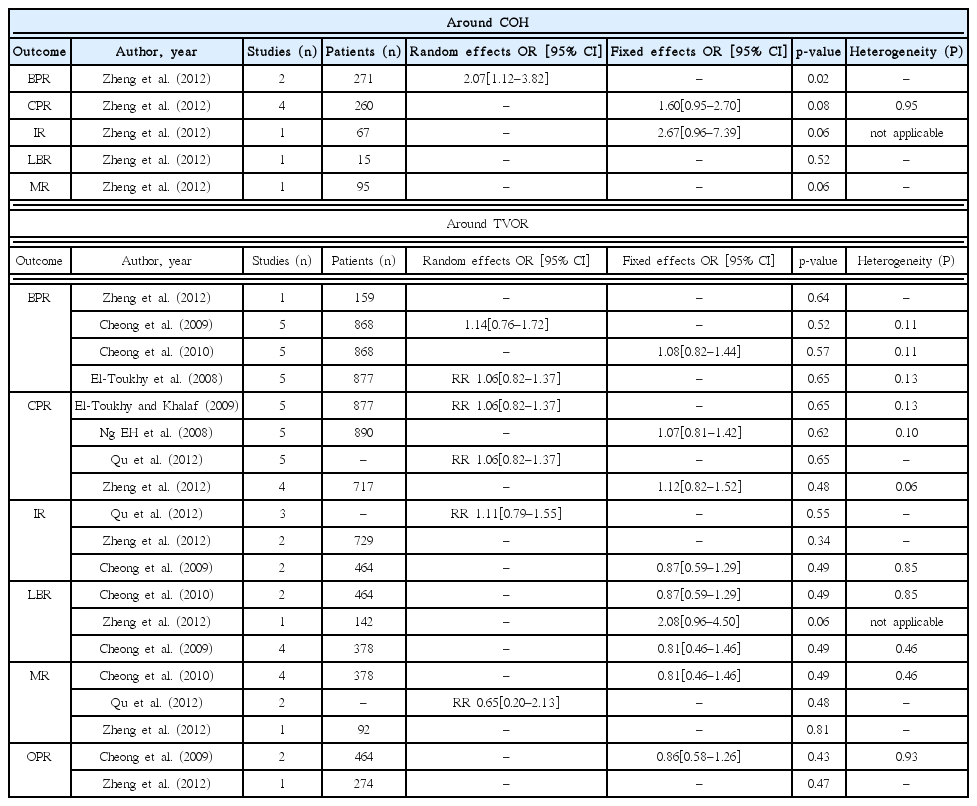
Main Outcomes of Meta-analyses Around COH and TVOR
In 2012, Zheng et al. reported that the BPR was affected only when acupuncture was performed around the time of COH (studies: n=2; patients: n=271; OR: 2.07; 95% CI: 1.12–3.82), but the same review found no effect on CPR.
Eight SRs reported that acupuncture at the time of TVOR had no significant effect.
Outcomes of Acupuncture around the Time of ET (Table 4)
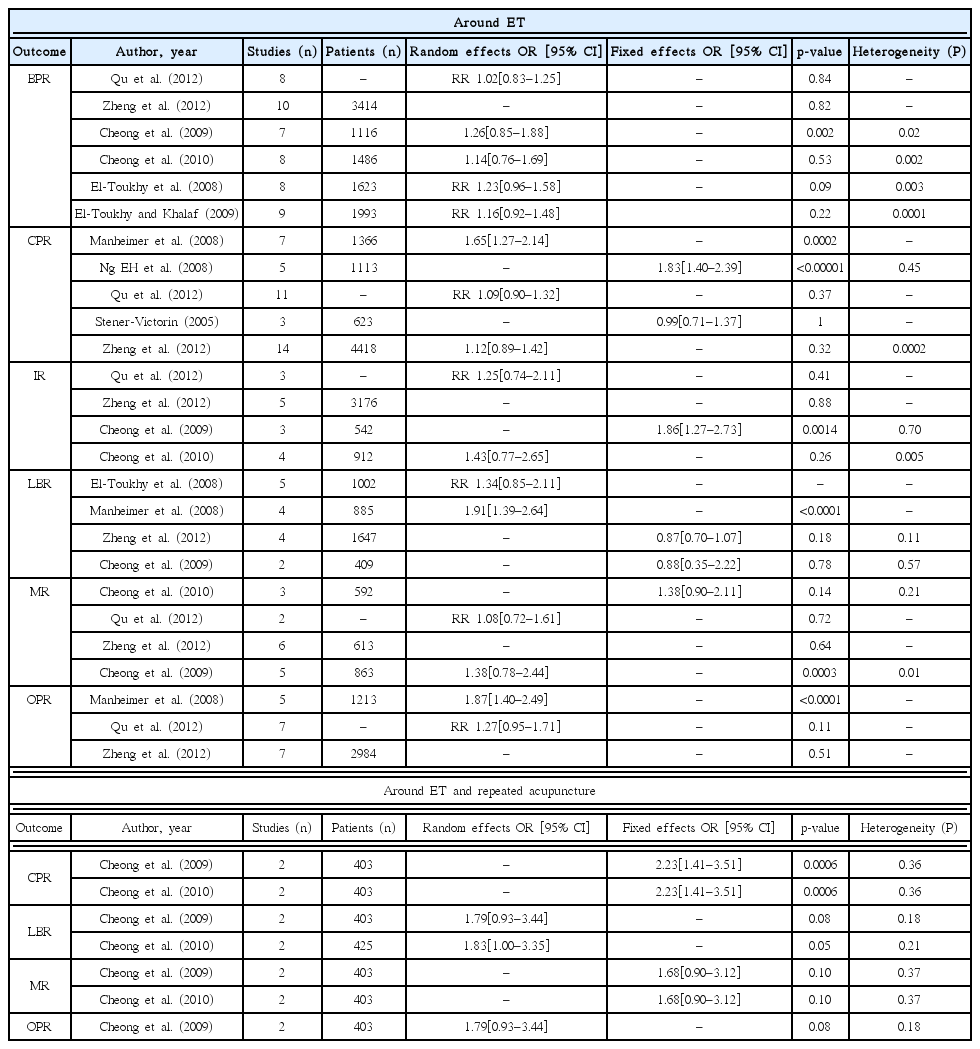
Main Outcomes of Meta-analyses Near the Time of ET
In seven SRs, acupuncture performed around the time of ET was reported to have a significant effect on the CPR, OPR and LBR. A significant impact on the CPR was reported by Cheong et al. (2008; OR 1.50, 95%; CI, 1.15–1.95), Manheimer et al. (2008; OR: 1.65; 95% CI: 1.27–2.14) and Ng et al. (2008; OR: 1.83; 95% CI: 1.40–2.39). Additionally, in 2008, Cheong et al. and Manheimer et al. reported a significant effect on the LBR (OR: 1.86; 95% CI: 1.27–2.73 and OR:1.91; 95% CI: 1.39–2.64, respectively).
Both Cheong et al. in 2008 and Manheimer et al. in 2008 reported a significant impact on the OPR (OR: 1.83; 95% CI: 1.32–2.53 and OR: 1.87; 95% CI: 1.40–2.49, respectively). However, the BPR, IR and MR were not significantly affected.
The results of repeated acupuncture after ET were evaluated in two SRs (Cheong et al. in 2008 and 2010). As both SRs included the same primary studies, they CPR outcomes results were the same (OR 2.23, 95% CI 1.41–3.51).The MR, OPR and LBR were not significantly affected.
Outcomes of Good-quality SRs
Five SRs12,17,19,22,24) were considered good-quality because they had 80 or more conversion points, few or no methodological shortcomings and a low risk of bias. The conclusions from the good-quality SRs and all SRs were not different.
Adverse Effects
The adverse effects of acupuncture were documented in 5 SRs. Anderson et al. (2007; 11 primary studies) and Manheimer et al. (2008; two of seven primary RCTs) reported no adverse events. In 2008 and 2010, Cheong et al. reported the experiences of patients in a trial by Smith et al. in 2006.27) The most frequently reported outcome in that trial was relaxation. Subjects in the control group, who did not receive acupuncture, reported being more relaxed than the study group. In 2012, Zheng et al. reported no significant differences between the acupuncture and control groups in the various MR comparisons. None of the 24 trials reported evidence of ovarian hyperstimulation or any treatment side effects.
Discussion
Summary of the Results
The recent high volume of trials and SRs studying the effect of adjunct acupuncture on the success rate of IVF has resulted in confusing and even conflicting conclusions. In the analysis of nine of the 11 previous SRs that involved meta-analyses, the pooled CPR of the acupuncture group was significantly higher than the CPR of the control group for the total IVF procedure. When performed around the time of ET, acupuncture significantly affected the CPR, OPR and LBR. Additionally, acupuncture performed around the time of COH and repeated two or three days after ET had a positive impact on the acupuncture group; however, the outcomes were limited due to an insufficient number of primary trials and the limited sample size (the results were derived from only two trials).
Most of the primary studies included in the good-quality SRs were included in all of the SRs. Two recent SRs published in 2012 (Qu et al. and Zheng et al.) covered studies performed since 2008, and relatively large numbers of trials were included (17 and 24 trials, respectively). While the results of these two recent SRs were not notably different from the results of the previous SRs, the recent SRs documented more types of success rates and also included the outcomes of COH.
We further evaluated the primary trials that were included in the good-quality SRs; 14 of 24 primary trials published between 1999 and 2009 were included in most of the five SRs. The remaining ten trials were performed between 2007 and 2011. The results of the more recent trials were not remarkably different from the results of the older trials, which suggests that the impact of acupuncture has not changed over time.
Limitations
The limitations of this overview include the heterogeneity of the individual trials and the SRs resulting from a wide range of various factors (i.e., differences in the acupuncture rationale and practice, the acupoints used, the control used, the number of acupuncture sessions, the timing of acupuncture relative to the IVF procedure and the outcome measures). Acupuncture controls are highly variable and can be categorised into 11 categories, including non-treatment, complementary control, sham acupuncture, nonspecific site control, minimal acupuncture, superficial acupuncture, and placebo needle control.28) It is difficult to establish a reasonable control in clinical trials involving acupuncture. Streitberger controls and sham acupuncture appear to be improper controls for acupuncture.24,29) In addition, the diversity of controls makes combining results difficult.
The lack of a convincing effect on LBR weakens the clinical implications because this measure is arguably the most important outcome for IVF patients.
SRs are prone to publication bias within the primary research data, which can also affect the SRs.30) Thus, the design of this study an overview of systematic reviews may also be affected by publication bias. The risk of publication bias is even greater because of the language restriction. In our methodology, only English and Korean SRs were included; however, some of the SRs included primary studies in Chinese. For instance, Zheng et al. (2012) covered acupuncture around the time of COH and included studies in Chinese and Taiwanese journals. Literature searches in Chinese may be necessary to draw thorough conclusions.
There was a considerable amount of temporal bias in this study because there were a greater number of older primary studies than recent studies. Some of the primary studies may be over-represented. In particular, some primary studies, especially the top 12 cited studies, were included in more than six SRs.
In their review from 2008, Manheimer et al. did not clearly document the references for their primary studies, and the specific reference for one primary study was unclear. Researchers must be cautious when using the list of primary studies included in an SR.
Perspective and Beyond
The mechanism of acupuncture’s effectiveness in IVF is believed to be related to the relief of emotional stress, an increase in blood flow to the pelvic cavity and the functional control of the hypothalamic-pituitary-ovarian axis.9) The improvement of the outcomes of ET with acupuncture is associated with the relief of stress and anxiety.9) On the day of ET, the patient is subjected to excessive emotional stress, which lowers the pregnancy rate.31) Acupuncture before and after ET relieves the stress associated with ET and may improve the pregnancy rate, possibly because acupuncture reduces vasoconstriction and improves uterine receptivity.32)
Consecutive acupuncture treatments after ET appear to be partially effective in increasing the CPR according to evidence from previous studies. However, the outcome measures are not reflected in the LBR, which is the most important result for IVF. Traditional Korean medical practitioners are cautious not to conduct excessive acupuncture on pregnant women to stabilize a human embryo. Therefore, in practice and research it may not be beneficial with respect to the LBR to conduct acupuncture procedures after ET.
Conclusion
In conclusion, there is conflicting evidence regarding the efficacy of adjunct acupuncture in IVF procedures; however, when analysing the full IVF procedure, some reviews have found an increased CPR following acupuncture. In particular, acupuncture performed around the time of ET has been shown to positively impact the CPR, LBR and OPR. There was insufficient evidence to conclude that acupuncture performed around the time of COH or repeated acupuncture two or three days after ET has a significant effect. Additionally, acupuncture performed around the time of TVOR had no positive effect on the pregnancy rate following IVF. There were no significant adverse effects, suggesting that there are no specific risks of adjunct acupuncture related to IVF.
Acknowledgements
The research described in this paper was supported by the Korea Health Promotion Foundation (Grant number A0100912A00). This grant was awarded to Se-Myung University, Department of Oriental Obstetrics and Gynecology, 837 Bongbang-dong Chungju-city, Chungcheongbuk-do, South Korea.