Long-term Survival of a Hepatocellular Carcinoma Patient Treated by Korean Medicine Combined with Western Therapy: a Case Report
Article information
Abstract
Objectives
Hepatocellular carcinoma patients have a poor prognosis and survival beyond 5 years is very rare in spite of western treatment. We report a case of long-term survival of a hepatocellular carcinoma patient treated by Korean medicine combined with western therapy.
Methods:
The treatment was provided from November 2004 to July 2012. Herbal medicine, acupuncture and moxibustion treatment were used as main treatment methods. We prescribed herbal medicines three times a day and performed acupuncture and moxibustion an average of 2–3 times a week. Clinical laboratory tests were performed each month and a CT scan was carried out 13 times during the treatment period. In order to evaluate the disease status, we checked the patient’s abdominal circumference, weight change and subjective symptoms regularly.
Results:
During treatment, subjective symptoms of the patient and state of ascites due to hepatocellular carcinoma were relatively stable. The progress of hepatocellular carcinoma was gradual without worsening rapidly. Since the initial diagnosis with hepatocellular carcinoma, the patient survived for a further 7 years and 9 months treated by Korean medicine combined with western treatment.
Conclusions:
According to the above results, this case indicates that Korean medical treatment combined with western therapy for hepatocellular carcinoma patients has synergistic effects of prolonged survival, relief of symptoms and management of complications.
Introduction
Hepatocellular carcinoma accounts for approximately 6% of all human cancers and it is estimated that almost one million new cases are diagnosed annually.1 Hepatocellular carcinoma is currently the fifth most common solid tumor worldwide and the fourth leading cause of cancer-related death.2
The vast majority of hepatocellular carcinomas worldwide (80%) are attributed to the hepatitis B (HBV) or hepatitis C virus (HCV), however, other risk factors include alcohol abuse, hemochromatosis, fatty liver disease, androgenic steroid use and other metabolic disorders.1,2
At present, hepatectomy and liver transplantation remain preferred methods to treat primary liver cancer.3 However, only a minority (20–25%) of hepatocellular carcinoma patients can be managed with curative treatment.4
Many patients cannot be treated surgically because of the advanced stage of the tumor and/or coexisting cirrhosis. Even for those patients who undergo resection, the recurrence rates can be as high as 50% in 2 years.5 Patients are mostly given palliative support care, transarterial chemoembolization (TACE) or systemic chemotherapies. However, hepatocellular carcinoma is well known to be a highly chemoresistant tumor, and the response rate is <10–20%.6 The overall median survival rate of untreated hepatocellular carcinoma is 3 months, and the 1-year survival rate is only 7.8%.7
Length of survival depends largely on the extent of cirrhosis in the liver; cirrhotic patients have shorter survival times and more limited therapeutic options. Portal vein occlusion, which occurs commonly, portends an even shorter survival. Complications from hepatocellular carcinoma are those of hepatic failure; death occurs from cachexia, variceal bleeding or malignant ascites.
The prognosis of ascites due to hepatocellular carcinoma is very poor. If hepatocellular carcinoma patients have malignant ascites, it is known that the mortality rate within 3 years is 50%.8
In this study, we report a case of hepatocellular carcinoma with malignant ascites in a 72-year old male. This patient survived over 7 years while under persistent treatment with Korean and western medicine.
Case Report
In November 2004, a 72-year-old man with a history of hepatitis C-related cirrhosis was referred to our hospital for lassitude and abdomen discomfort. That October, hepatocellular carcinoma of the right lobe of the liver had been diagnosed and he underwent transarterial chemoembolization (TACE) once at the National Cancer Center.
On visiting our hospital, a previous enhanced computed tomography (CT) scan (done in October 2004) revealed about 5.3cm in S5, 7, 8, which was enhanced in the arterial phase and washed out in the equilibrium phase, which is typical of hepatocellular carcinoma (this is based on copies of a patient’s medical records). Portal vein thrombosis of the 2nd branch of the right portal vein, liver cirrhosis with gastroesophageal varices and mild peritoneal ascites were observed. There were no abnormalities on chest radiographs. Laboratory tests revealed slight elevation of AST, ALT, ALP and AFP. All other blood parameters were in normal ranges (Table 1). His Child-Pugh score was class B, and the tumor stage was stage IIIA (T3N0M0) based on the general rules for the study of primary liver cancer.9 He presented with lassitude and intermittent abdominal pain. His performance status was relatively mild.
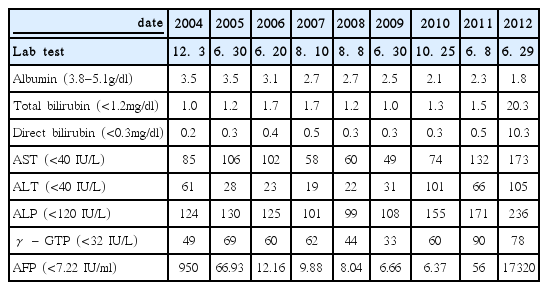
The Serial Change of Lab Findings
Between November 2004 and July 2012, he was admitted to our hospital 30 times and underwent outpatient treatment a total of 315 times. The mean length of hospitalization was 24.24 days and outpatient treatment was performed on a roughly monthly basis. During this period, we prescribed herbal medicines three times a day and applied traditional acupuncture and indirect moxibustion regularly.
Following this Korean treatment, various herbal medicines were selected by the Korean medical doctor’s diagnosis. The herbal medicines were summarized as follows; Chuunggan-tang (CGT), Myeonyeok-dan (PSM), Hamam-dan (HAD), Jakyakgamcho-tang, Woohwanggusa-dan, Gamibunrieum, Bojungchisem-tang, Saengkankunbi-tang, O-Ryoung-San, etc. (Table 2). Among these medicines, Chuunggan-tang (CGT) and Hamam-dan (HAD) were mainly prescribed. Chuunggan-tang (CGT) is a new herbal formula modified from In-Jin-O-Ryoung-San which has been a standardized formula for liver injury related jaundice for several centuries (Table 3).10 Hamam-dan (HAD) has shown antitumor, immune enhancing, antiangiogenic and antimetastatic effects in vitro and in vivo.11 It consists of eight herbs (botanical names, dosage per one capsule (250mg) (Table 4).12 We also performed acupuncture and moxibustion 2-3 times each week on average. Acupoints were chosen depending on chief complaints of the patient. Acupuncture points in this treatment were as follows: LU-7, LU-9, LU-10, LI-6, LI-4, ST-42, LR-1, LR-2, LR-3, LR-5, LR-13, LR-14, SP-3, SP-4, HT-8, BL-7, KI-6, KI-9, KI-10, PC-6, GB-39, GV-20, GV-23, CV-3, CV-4, CV-6, CV-9, CV-12, CV-13, CV-15, and CV-17. Acupoints of moxibustion were CV-4, ST-25, and CV-12.
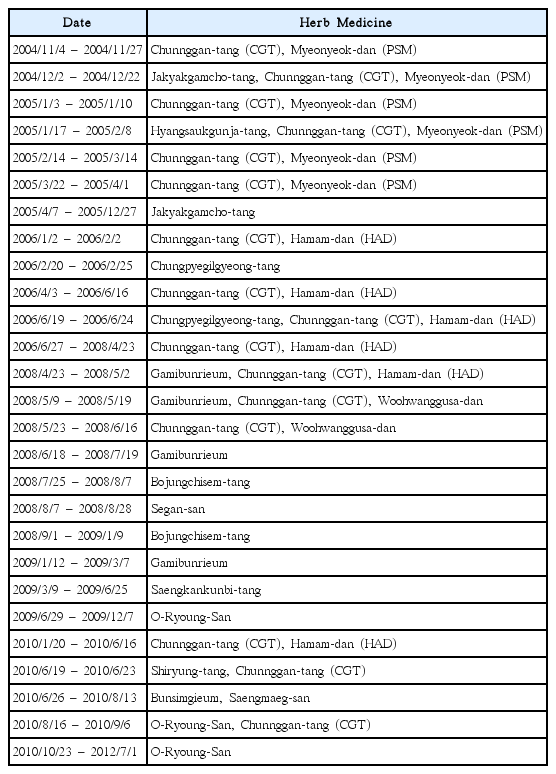
Herb Medicine Treatment
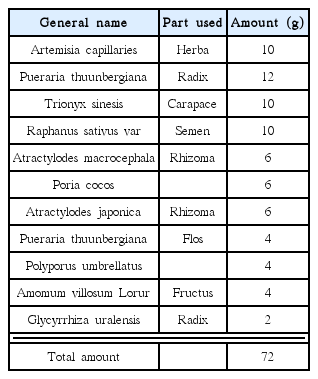
Prescription of Chunnggantang (CGT)

Prescription of Hamam-dan (HAD)
In April 2005, CT scan revealed recurred lesions in the liver and he received transarterial chemoembolization (TACE) (Fig. 1A), but his condition was mild. In April 2006, a follow-up of CT scan showed recurred lesions, but after a few months, he heard that there were no specific lesions in the liver and status of ascites was no interval change (Fig 1B). During this period, he complained of intermittent cough, sputum and knee pain. Until March 2007, his status was very mild, but CT scan in March 2007 revealed viable tumors in the liver and he underwent additional TACE. From November 2007 to March 2008, he underwent TACE three further times and received proton therapy 22 times from January to February of 2008. In April 2008, his condition worsened. His body weight and abdominal circumference began to increase (Table 5), so he started taking diuretics from this point. CT scan in September 2009 showed no interval change of the liver (Fig. 1C) and during this period, symptoms related to hepatic encephalopathy appeared frequently. CT scan was performed in September 2010 and showed multiple viable tumors in S3, S8 of the liver (Fig. 1D), so he received additional TACE. In March 2011, follow-up of CT scan revealed recurred lesions in S8 dome, S2, S6 and a large amount of ascites (Fig. 1E). His condition deteriorated and status of ascites became worse. CT scan in March 2012 showed increased size of tumor at the liver S8 dome and ascites in the peritoneal cavity (Fig. 1F). The result of LFT and AFP was high in July 2012 (Table 1). In that month, he expired due to tumor progression.

Fig. 1: CT images
Fig. 1A: CT (in April 2005) showing recurred lesions of cancer in right lobe of liver.
Fig. 1B: CT (in April 2006) showing recurred lesions of cancer in S8 dome, S5, S7
Fig. 1C: CT (in September 2009) showing no interval change of multiple compact lipiodol retention nodules, both hepatic lobes.
Fig. 1D: CT (in September 2010) showing multiple viable tumors in liver S3, S8 and small amounts of ascites.
Fig. 1E: CT (in March 2011) showing recurred lesions in S8 dome, S2, S6 and large amounts of ascites.
Fig. 1F: CT (in March 2012) showing increased size of tumor at liver S8 dome and ascites in peritoneal cavity.

The Change of Abdominal Circumference and Body Weight
Since the first diagnosis with hepatocellular carcinoma, he survived for 7 years and 9 months treated with Korean medicine combined with western therapy (from November 2004 to July 2012).
Discussion
Hepatocellular carcinoma is a malignancy of the hepatocyte, generally leading to death within 6–20 months.1 Hepatocellular carcinoma frequently arises in the setting of cirrhosis, appearing 20–30 years following the initial insult to the liver. However, 25% of patients have no history or risk factors for the development of cirrhosis. The extent of hepatic dysfunction limits treatment options, and as many patients die of liver failure due to tumor progression.
Median overall survival for advanced-stage disease in patients with good performance score and preserved liver function reserve is still less than 1 year, even with treatment.6
If hepatocellular carcinoma patients have malignant ascites, the prognosis is poorer. The presence of malignant ascites is a grave prognostic sign. It is well known that the 3-year survival rate of patients with malignant ascites is <50% and the survival rate in this patient population is poor, averaging about 20 weeks from time of diagnosis.13
In the present case, the patient had been diagnosed with liver cirrhosis, hepatitis C infection, which reveals low liver function. In addition, he had mild abdominal ascites on initial diagnosis.
Accompanied with malignant ascites, the status of hepatocellular carcinoma patients becomes worse and the survival period shortens.13 In contrast, the state of this patient’s ascites remained very stable from November 2004 to April 2008. Since April 2008, he had been prescribed diuretics, but which were only used intermittently or supplied at 1/3–1/2 of usual dosage. Despite low dosage diuretics, we could see maintenance of ascites without rapid increase.
During the Korean medical treatment period, the patient underwent transarterial chemoembolization (TACE) seven times and received proton therapy 22 times. According to recent study, the prognosis of patients with hepatocellular carcinoma undergoing TACE is not very good: mean survival was 13.98 months and the 3-year survival rate is only 20%.14 Remarkably, the patient in this case survived for 7 years and 9 months in spite of recurrence of hepatocellular carcinoma and malignant ascites. In addition, his condition and symptoms were managed without severe complications until June, 2008. From June 2008, his condition worsened and symptoms related with encephalopathy presented intermittently. From this point, his laboratory data began to be unstable. Nevertheless, his overall condition and symptoms were managed relatively well. His status had remained relatively mild until April 2008, when he presented severe lower limb edema, abdominal distention and weight gain. In spite of ascites, his abdominal circumference and body weight were managed stable without rapid worsening (Table 5).
Although he expired in July of 2012 in our hospital, the long-term survival of this hepatocellular carcinoma patient was remarkable. The fact of management of malignant ascites without western therapy for 4 years was also notable.
According to the above results, this case indicates that Korean medical treatment combined with western therapy for hepatocellular carcinoma patients has synergistic effects of prolonged survival, relief of symptoms and management of complications.
Up to now, long-term Korean medical treatment in patients of hepatocellular carcinoma has not yet been reported in Korea. In this respect, our study is valuable for observation of a patient with clinical treatment over a long period.
Further, this case may trigger more long-term studies of hepatocellular carcinoma patients treated by Korean medicine combined with conventional treatment, clarifying its broader efficacy.