Successful Treatment of Two Patients with Immune Thrombocytopenic Purpura Using Herbal Decoction
Article information
Abstract
Objectives:
This case report was conducted to introduce the effectiveness of herbal decoction on patients with chronic immune thrombocytopenic purpura (ITP).
Methods:
We closely observed two patients who were admitted to the Department of Internal Medicine 1 of Kyung-Hee Korean Medical Hospital due to ITP. We gave a herbal decoction to these patients and then analyzed the changes in their general conditions as well as blood test results.
Results and Conclusions:
The treatment with herbal decoctions was helpful for ITP patients.
Introduction
Immune thrombocytopenic purpura is an acquired disorder. The two criteria required for its diagnosis are normal complete blood count and white blood cell differential, including a normal peripheral blood smear, and no clinically apparent associated conditions that may cause thrombocytopenia1).
The pathogenesis of ITP is thought to be related to increased platelet destruction with inhibition of platelet production through the production of specific autoantibodies. However, such antibodies are not demonstrable in all patients, and assays for antiplatelet antibodies have not been important for management decisions2).
The incidence of ITP is highest in children, and may be greater in boys than in girls3). In adults, the incidence increases with age. The incidence in women is greater than in men at the age under 60, but in adults age over 60, the incidence in men is the same as in women4).
When deciding to treat an ITP patient, a threshold platelet count of 30,000/microL for clinical decisions, rather than a range of platelet counts, is presented. However, clinical symptoms and patients’ concerns are more important for treatment decisions. Usually, glucocorticoids are the first line therapy, but IVIG (intra-venous immuno-globulin) may also be used as the first line instead of glucocorticoids when a more rapid increase in platelet count is required. After taking glucocorticoids, many patients may suffer from adverse effects such as weight gain, fluid retention insomnia, Cushingoid facies, dorsal fat, diabetes, osteoporosis, and so on5).
In addition to these ordinary therapies, herbal medicine can be effective in treating these patients. Now we report one child and one adult ITP patient who have shown improvement while taking herbal decoction.
Case Presentation
Case 1
(1) Name: Huh ○ ○, M/7
(2) O/S: 2010. 7.
(3) C/C: ① rhinorrhea from allergy rhinitis ② fatigue
(4) P/H: N
(5) F/H: N
(6) P/I: In July 2010, the patient’s platelet count was 30,000 when examined at Ewha Womans University Hospital. There, he was diagnosed with ITP and started to take glucocorticoid. He was injected with IVIG 3 times. The last treatment was done in July 2011. He also had visited a local Korean medicine clinic to take a herbal decoction, which was not effective.
(7) Treatment
① Jiyuseongyangtang (JYSYT-地楡升陽湯)1 - 1ch#3, 50cc (Table 1)
② Acupuncture: N
(9) Lapse
① Duration of treatment: 2011. 09. 30 ∼ 2013.02.26
-
② Laboratory data

Change of platelet count (10^3/μL) of the child patient
Case 2
(1) Name: Nam Kung ○, M/21
(2) O/S: 2010. 9
(3) C/C: ① purpura ② petechiae
(4) P/H: Admission to local hospital for about 1 month due to a car accident when 10 years old.
(5) F/H: Father HTN
(6) P/I: In September 2010, he found several purpura lesions on his skin and visited a local dermatologic clinic. The doctor advised him to get a thorough medical examination at another, bigger hospital. He went to Seoul St. Mary’s hospital and was diagnosed with ITP. At that time, his platelet was 5,000 10^3/μL and he started to take glucocorticoid.
(7) Treatment
① Jiyuseongyangtang (JYSYT地楡升陽湯)2 - 2ch#3, 100cc (Table 2)
② Acupuncture: N
(9) Lapse
① Duration of Treatment: 2011.05.31 ∼ 2013.03.04
-
② Laboratory data
Change of platelet count (10^3/μL) of the child patient
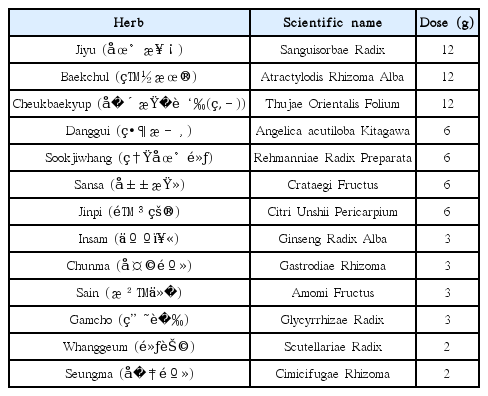
Jiyuseongyangtang(JYSYT-升麻)1-1ch#3, 50cc
Change of platelet count (10^3/μL) of the child patient
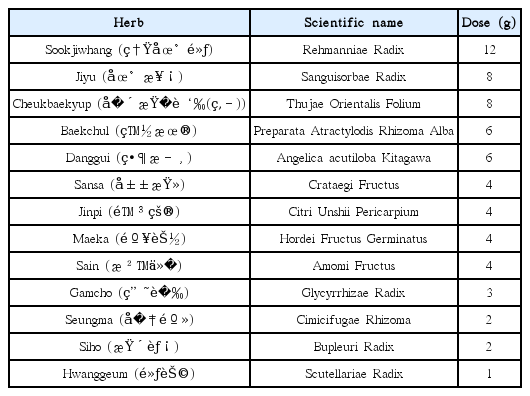
Jiyuseongyangtang(JYSYT-陰)2-2ch#3, 100cc
Change of platelet count (10^3/μL) of the child patient
Treatment results
There is no gold standard test that can confirm ITP. The diagnosis is a consequence of exclusions, which requires that other causes of thrombocytopenia be ruled out. A presumptive diagnosis of ITP is made when the history, physical examination, complete blood count, and examination of the peripheral blood smear do not suggest other causes for the patient’s isolated thrombocytopenia1.
Two patients were diagnosed as ITP at other university hospitals. When they came to Kyunghee Korean medicine hospital, both of them submitted medical certificates diagnosed with ITP. Since ITP appears only with abnormal platelet counts, we regularly checked only CBC counts of each patient while we gave herbal decoctions.
The 5-year-old child patient was 123cm tall and weighed 25kg when he first came to our clinic. He had normal appetite, bowel and urine habits. However, he frequently complained about rhinorrhea from allergy rhinitis, fatigue, and bad feelings at every seasonal changing time. His face was pale, and pulse was weak, thin, and quite tight. He had been tapering off prednisolone to 2.5 mg qd. We prescribed him JYSYT1 (table 1) from September 23, 2011. We divided 1 chup (帖) into 3 packs (包) for this 5 year-old boy, adjusting the concentration of the decoction to be milder than for an adult patient. His platelet count started to rise once he started taking this medicine. This rising tendency continued for about 3 months, despite him quitting prednisolone on February 3, 2012. However, after suffering from a severe cold in September 2012, his platelet count dropped again to around 80,000 for a couple of months. When we examined his platelet count on January 7, 2013, it was 180,000, which was already over the normal limit.
The adult patient was 178cm tall and weighed 69kg. He had normal appetite and urine habits. He had sporadic constipation, and often suffered from dyspepsia. Once he decided to take herbal medicine, he quit taking prednisolone and concentrated on our therapy. We prescribed him JYSYT2 (Table 2) from February 15, 2011. We divided 2 chup (帖) into 3 packs (包). Though his platelet count had fluctuated during treatment, the overall tendency had been gradually rising, and the final platelet count was 162,000 at February 23, 2013.
Discussion
The pathogenesis of ITP is related to a combination of increased platelet destruction along with inhibition of megakaryocyte platelet production via the production of specific IgG autoantibodies by the patient’s B cells, most often directed against platelet membrane glycoproteins such as GPIIb/IIIa2,6,7).
ITP is a common acquired bleeding disorder. The incidence of ITP in children is greater than the incidence among adults8).
Understanding of the natural history of untreated ITP, which differs between children and adults, provides part of the rationale to decide which patients should be treated. Many children receive no specific therapy, since 70 to 80 percent have a spontaneous complete remission of the disease within six months.
Approximately 70 percent of children have the acute form of ITP, which is defined by recovery of presentation within six months with or without treatment. Pharmacologic intervention, when used, is directed toward the early control of symptoms, such as stopping severe hemorrhage or minimizing the risk of significant bleeding. Such therapy does not affect the long-term outcome9,10).
ITP in adults is typically a chronic disease, the prevalence exceeds the incidence. In one estimate of the prevalence of ITP in the US, the estimate was approximately 100 per million per year, with age cohorts ranging from 41 to 160 per million per year, with the highest values seen in the oldest cohort11).
Spontaneous remissions are unusual in adults, occurring in 9 percent in one series. The necessity for treatment in adults varies with the severity of the thrombocytopenia12).
The incidence of major bleeding and death from bleeding is also unknown, although these events are thought to be rare. The absence of firm data on these important clinical outcomes hinders all management decisions12,13,14).
Since major bleeding is rare and primarily occurs in those with platelet counts below 10,000/microL15), the goal for treatment of ITP is to provide a safe platelet count to prevent major bleeding, rather than returning the platelet count to normal16,17,18).
However, the rationale for continued therapy is uncertain among asymptomatic patients with chronic severe thrombocytopenia who have had no or only a partial response to one or more treatment regimens. Unnecessary treatment of asymptomatic patients with mild to moderate thrombocytopenia, platelet count greater than 30,000/microL, should be avoided, because ITP may be a more benign disease than previously thought, and may be best approached by a conservative treatment program in the majority of patients19).
Treatment to increase the platelet count is always initiated in patients with a platelet count below 30,000/microL, which is severe enough to constitute a risk of bleeding. Glucocorticoids are the preferred agents for first-line therapy, while splenectomy, rituximab, and thrombopoiesis-stimulating agent s are typically reserved for second or third-line therapy20,21,22).
When approaching children ITP, the ASH guidelines (published in 1996) suggest that no therapeutic intervention is generally needed for children with platelet counts greater than 30,000/microL as they are unlikely to have serious bleeding. Pharmacologic therapy is recommended for any child with significant bleeding regardless of the platelet count and with platelet counts less than 10,000/microL and cutaneous bleeding23).
Unlike in western medicine, there is no specific term or definition which refers to ITP in Korean medicine. However, in Donguibogam (東醫寶鑑) there are some records describing purpura or petechia24). It also says that these features seem to be related to weak spleen (脾虛), shrunken yin (陰虛), and heated blood (血熱). These states are all associated with blood flow. From this point of view, they already have understood this phenomenon as the malfunction of blood cells or a disorder of the blood stream25).
Therefore, the goal of treating ITP is not only preventing bleeding and bruising but also recovering normal platelet count, taking care of each patient’s individual conditions.
Both patients’ prescriptions were based on JYSYT. The fundamental decoction of JYSYT is Ikweeseongyangtang (IWSYT, 益胃升揚湯). We added Sookjihwang (熟地黃) to raise yin (陰) and blood (血), and increased Jiyu (地楡) to prevent bleeding signs. IWSYT consists of Bojungikgitang (BJIGT, 補中益氣湯) and Hwanggeum (黃芩), and BJIGT is a famous prescription for those who are lacking in ki (氣虛). We thought the major cause of ITP for these two people was weak spleen (脾虛).
We used JYSYT1 to the child patient. His ki (氣) was so insufficient that he was sensitive to seasonal changes, complained about fatigue, and frequently caught cold. His pulse was weak and thin. This is why we put more Baekchul (白朮) and added Insam (人參).
We gave JYSYT2 to the adult patient. We put in more Sookjiwhang (熟地黃) than the child patient, because we thought he had shrunken yin (陰.) He sweated while sleeping, his cheek turned pink when he was tired or talking, and felt intermittent thirst. We also put in a small amount of Siho (柴胡) to bring down this mild heat (陰虛熱).
There are other reports which describe the effectiveness of herbal decoctions in ITP patients허 All the cases showed improvements whether parallel therapy with glucocorticoid was done or not27,28,29). However, the starting point of rising platelet count seems to be shorter in those who did not use glucocorticoid.
Since there is only a small chance to encounter ITP patients in local Korean medicine clinics, we must demonstrate the effectiveness of herbal medicine from just a few case reports. This report is also made to let people know the high possibility of herbal decoction in treating ITP patients. From this point of view, lack of number of patients is a limitation to generalizing to all kinds of ITP patients. Therefore, we should continue to study this disease through experiments in vivo or in vitro. We should investigate the specific steps, clarifying how platelet disorders recover to normal stage. After that, a clinical research should be prepared to prove these experiments. Since we have seen that herbal decoction can be a good remedy to ITP patients, regardless of age and sex, we hope that further study can be carried out soon.