Correlation between Abdominal Fat Distribution and Abdominal Temperature in Korean Premenopausal Obese Women
Article information
Abstract
Objectives:
Considering that homeothermy is a major component of metabolic rate, body temperature might play a role in the pathophysiology of obesity. This study aimed to determine the relationship between abdominal fat distribution and abdominal temperature in Korean, premenopausal, obese women.
Methods:
Weight and height were measured in 26 premenopausal, obese women to calculate body mass index (BMI). Obesity was defined as a BMI ≥25kg/m2. Waist circumference (WC) was also measured as well as abdominal fat by computed tomography (CT) and abdominal temperature by digital infrared thermographic imaging (DITI).
Results:
Visceral abdominal fat area was found to have a significant negative correlation with the temperature of Guanyuan (CV4, lower abdomen acupoint). We also found the visceral-subcutaneous fat ratio had a significant negative correlation with the temperature of CV4 and Right Tianshu (RST25, lateral navel acupoint). Only visceral fat and its ratio to subcutaneous fat had a significant correlation with abdominal temperature. Subcutaneous fat area and total fat area were not correlated with abdominal temperature.
Conclusions:
This study suggests that abdominal visceral fat has a significant negative correlation with abdominal temperature. Further study is needed to uncover the relationship between abdominal fat distribution and temperature regulation in obese individuals and to define the role of body temperature in the pathogenesis of obesity.
Introduction
Although the global obesity epidemic and its associated health consequences have aroused interest in the root causes of excessive fat accumulation in adipose tissue1), no definite mechanisms have been identified. The common explanation that obesity is the result of overeating or limited physical activity is time honoured, but this hypothesis oversimplifies the complexity of the problem2), as it has been demonstrated that lean and obese individuals differ in their metabolic efficiency3). Considering that metabolic rate is important in energy output and homeothermy is a major component of resting metabolic rate (RMR), body temperature may play a role in the pathophysiology of obesity4).
Currently, some data5–7) support an inverse association between core temperature and obesity, while other data do not8–9). Studies involving different populations have provided considerable evidences for significant variations in both RMR and core temperatures10–13). In one study on the relationship between adiposity and regional body temperature, core temperature did not differ significantly between lean and obese subjects. In another study, digital infrared thermographic imaging (DITI)-measured abdominal skin temperature was significantly lower and fingernail-bed temperature was significantly higher in obese subjects than in lean subjects, suggesting that greater subcutaneous abdominal fat in the obese may provide a significant insulating layer that blunts abdominal heat transfer, and that augmented heat release from the hands may offset heat retention14). However, most studies on DITI-measured abdominal temperature that simply compare obese and non-obese subjects do not reflect the extent and the distribution of subcutaneous and visceral (intra-abdominal) fat15–16).
The purpose of this study was to determine whether abdominal fat distribution affects abdominal temperature in Korean premenopausal obese women.
Methods
1. Participants
Participants were recruited through announcements and advertisements in newspapers and on hospital websites. 30 obese (BMI ≥25kg/m2) Korean women between 18 and 55 years of age were enrolled in the study from 1 July to 30 October 2011, after providing written informed consent. Participants had to be ambulatory, 18 to 55 years old, and have a body-mass index (BMI) ≥25 kg/m2. Participants were excluded if they previously or currently had heart disease, hypertension, diabetes mellitus, kidney disease, or malignant tumors. Also excluded were smokers and participants who had experienced weight changes over 3 kg within the past 2 months, who received any treatment for obesity in the past 6 months, who were or might be pregnant or who had given birth in the last 6 months. Based on these exclusion criteria, we excluded 4 women (1 for hypertension, 1 for hydronephrosis, 2 for previous obesity treatment), resulting in a sample population of 26 women (Fig.1). To avoid the effect of menopause on abdominal fat and body temperature, we included only premenopausal women. This study was approved by the Institutional Review Board of Kyung Hee University Hospital at Gang-dong.
Schematic diagram of study design.
Schematic diagram of study design. Thirty participants were recruited, and 4 subjects were excluded by exclusion criteria. Results of 26 women were analyzed.
2. Evaluation
1) Anthropometry
Body weight and height were measured to the nearest 0.1 kg and 0.1 cm, respectively. Waist circumference (WC) was measured by one observer, using the same tapeline, and was performed three times according to the World Health Organization (WHO) method, at mid-point between the lower end of the rib cage and top of the iliac crest in a standing position, which is usually 3 cm above the anterior superior iliac spine17).
2) Abdominal Fat Computed Tomography (CT) Scanning
Abdominal fat area was measured by CT scanning (Gemini 16 Power CT, Phillips Medical Systems, Cleveland, OH, USA) between the L4 and L5 vertebrae levels in a standing position18). Cross-sectional total fat area (TFA) and visceral fat area (VFA) were estimated by delineating the regions and calculated at an attenuation range of −190 to −30 Hounsfield units (HU).
3) Digital Infrared Thermographic Imaging (DITI)
Abdominal temperature was measured by DITI (IRCT-510, Dong Seo Corporation, Su-won, Korea) at a consistent room temperature (25 °C) and humidity, with light and heat blocked from the outside.
To rule out other factors that may affect the thermographic image, 24 hours prior to measurement, irritations that could change body temperature, such as other treatments, medications, caffeine, alcohol, and exercise, were restricted. To improve measurement accuracy, participants waited 15 minutes in a quiet room at room temperature before the measurements began. A thermographic image was taken in a standing position. To minimize the effect of circadian rhythm, the DITI was performed during the afternoon for all participants19–20).
Temperature measurement sites were chosen among acupuncture points cited in other studies21–22), and we designated 1cm2 square test locations in the upper abdomen (Zhongwan, CV12), lower abdomen (Guanyuan, CV4), and lateral abdomen (Tianshu, RST25 and LST25) (Fig.2). The temperature inside each square was measured three times and a mean value was calculated.
Acupuncture point locations.
Acupuncture point locations. (a) CV 4, Guanyuan, (b) CV 12, Zhongwan, (c) ST 25, Tianshu. This figure originated from the World Health Organization Standard Acupuncture Point Locations.
Guanyuan (CV4), the 4th meridian point of the conception vessel (CV), is located on the lower abdomen, at a point 3/5 down the ventral midline connecting the umbilicus to the pubic tubercle. Zhongwan (CV12), the 12th meridian point of the CV, is located on the upper abdomen, at the midpoint of the line connecting the xiphisternal junction and the center of the umbilicus. Tianshu (ST25), the 25th meridian point of the stomach meridian (ST), is located at 2 B-cun, lateral to the center of the umbilicus23).
4) Data analysis
All values are expressed as mean ± SD. Correlation between fat area and abdominal temperature was analysed by Spearman’s correlation using the Statistical Package for the Social Sciences (SPSS) version 12.0 program for windows. A p-value less than 0.05 was considered statistically significant.
Results
1. Demographic characteristics of participants
The 26 women were aged from 18 to 49 years and had a BMI range of 25.4 to 35.5 kg/m2. Participant demographics, anthropometric characteristics, and mean abdominal fat areas are summarized in Table 1. Mean abdominal temperatures by DITI are summarized in Table 2.
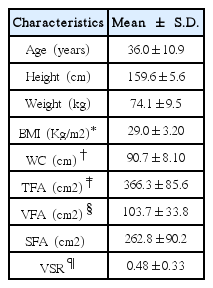
Participants Characteristics (n=26)
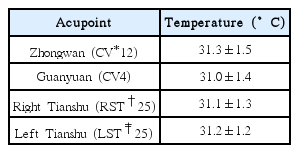
Mean Abdominal Temperature by DITI (n=26)
2. Abdominal fat and abdominal temperature correlation
Visceral fat area (VFA) was negatively correlated with the temperature at CV4 (R=−0.420, p=0.033). There were no significant correlations between VFA and the other temperature locations (CV12, RST25, LST25). Visceral-subcutaneous ratio (VSR) was negatively correlated with the temperature of CV4 (R=−0.450, p=0.021) and RST25 (R=−0.413, p=0.036). There were no significant correlations between VSR and the other temperature locations (CV12, LST25). Total fat area (TFA) and subcutaneous fat area (SFA) were not significantly correlated with any of the abdominal temperatures. Correlations between abdominal fat and abdominal temperature by DITI are summarized in Table 3. and Fig.3.
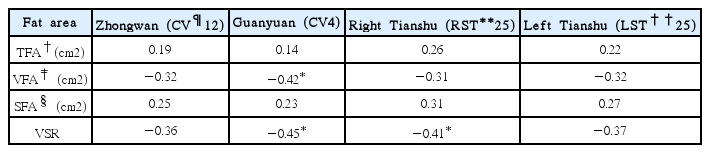
Correlation between Abdominal Fat Area and Abdominal Temperature (n=26)
Scatter graphs of correlation between abdominal fat and abdominal temperature.
Scatter graphs of correlation between abdominal fat and abdominal temperature. Visceral Fat Area (VFA) is negatively correlated with the temperature of CV4 (R=−0.420, p=0.033). Visceral-Subcutaneous Ratio (VSR) is negatively correlated with the temperature of CV4 (R=−0.450, p=0.021) and RST25 (R=−0.413, p=0.036).
Discussion
The aim of this study was to achieve a better understanding of body temperature in the pathophysiology of obesity by evaluating the relationships between the distribution of abdominal fat and abdominal temperature under the thermoneutral conditions in Korean premenopausal obese women. Several studies have found that obesity is associated with lower body temperature. In previous studies, obese subjects classified by BMI or fat mass had significantly low temperatures in the trunk or belly, and blunted cold-induced thermogenesis4,15–16,24–25), suggesting that the fat tissue has lower thermal conductivity and that the adipose tissue of obese individuals has lower blood flow26). These results also suggest that the low temperature may cause obesity by lowering metabolic rate or changing lipid metabolism4,27). However, these studies had limited discussion on the extent and the distribution of adipose tissue, and on whether abdominal temperature is more related to visceral or subcutaneous fat. Therefore, we conducted CT scanning to classify abdominal fat as visceral or subcutaneous fat. To our knowledge, this is the first study to demonstrate the relationship between the visceral abdominal fat and the abdominal temperature.
Our findings reveal that visceral fat has a correlation with lower abdominal temperature, while subcutaneous and total fat are not correlated with abdominal temperature. These results cast doubt on the assumption that the low thermal conductivity of fat is responsible for the low abdominal temperatures. If this assumption is correct, TFA and SFA would correlate with the abdominal temperature, however our results indicate that only visceral fat or its ratio is significantly correlated with abdominal temperature.
The primary role of adipose tissue is as a passive energy reservoir. The main function of white adipose tissue (WAT) is energy storage, whereas brown adipose tissue (BAT) produces heat. In all mammals including humans, most fat tissue is WAT located in various organs and parts of the body28–29). WAT is the main reservoir in mammals, and it serves as thermal and mechanical insulation. Recently, adipose tissue has been recognized as a dynamic endocrine organ, involved in broad metabolic processes. WAT secretes several major hormones, such as leptin and adiponectin, protein signals, and factors, such as adipokines, and is finally being recognized as an endocrine organ30).
The location and distribution of adipose tissue reveals its function. Subcutaneous adipose tissue is located underneath the skin and reserve body fat or acts as thermal insulation. Visceral adipose tissue is located between organs and secrets endocrine hormones such as leptin. It also releases non-esterified fatty acid (NEFA) directly into the portal system, thus increasing oxidative stress and insulin resistance. Hence, visceral adipose tissue has a greater effect on hepatic metabolic function than subcutaneous fat, and in turn, on systematic metabolism. In addition, it also secretes several unique adipokines and proinflammatory factors causing a chronic inflammatory state30–32). Visceral fat likely play a greater metabolic role that affects skin temperature than subcutaneous fat, as the latter serves merely as insulation.
Guanyuan (CV4), which showed a negative correlation with VFA and VSR in our study, is located at a point 3/5 down the ventral midline connecting the umbilicus to the pubic tubercle23). CV4 is reportedly related to gynaecological disorders and abdominal obesity. In Korean medicine, the conception vessel nourishes the uterus to adjust the body functions and CV4 is an important acupoint that reinforces qi and blood. In treatment, indications of CV4 include genitourinary and gynaecological disorders, and several deficiency syndromes33–34). As a main point that reflects the essential energy of the body, we expected that CV4 would correlate with metabolic visceral fat. Thus temperature of CV4 could be a possible tool for assessment of the visceral fat.
This study had several limitations. First, the sample size was too small to generalize our findings. Second, body temperature can vary by person, and even in one individual, results may vary depending on the season or other external factors. In future studies, assessment of body temperature should be done for a prolonged period, and mediating factors, such as fasting or low energy intake, should be assessed on both obese and lean individuals. Third, other factors that could affect body temperature such as basal metabolic rate (BMR), autonomic nervous system (ANS) activity, and body surface area were not considered in this study.
Other temperature sites, such as core temperature and distal skin temperature, should also be measured. Also, instead of simply comparing the subjects’ temperatures, a gap of temperatures between different sites (e.g. between anal and abdominal temperature) in one person, or the ability to control one’s temperature in different conditions could help explain homeothermy in the pathogenesis of obesity. Other diagnostic methods, such as blood tests or heart rate variability (HRV) testing, would also help us understand body temperature mechanisms (e.g. chronic inflammation state or imbalance of ANS) in the obese.
Conclusion
In order to study the correlation between the abdominal fat distribution and abdominal temperature, we conducted anthropometry, abdominal fat CT scanning, and DITI in 26 Korean premenopausal obese women aged from 18 to 49, BMI range from 25.4 to 35.5 kg/m2. We analyzed the correlation between abdominal fat distribution and abdominal temperature at 4 sites (CV4, CV12, RST25, LST25) using Spearman’s correlation, and the results are shown below.
VFA and the temperature of CV4 had a significant negative correlation. VFA and temperature of other points (CV12, RST25, LST25) had no significant correlation.
VSR and the temperature of CV4 and RST25 had a significant negative correlation. VSR and temperature of other parts (CV12, LST25) had no significant correlation.
Neither SFA and TFA had any significant correlation with abdominal temperature.
Our study suggests that lower abdominal temperature has a significant negative correlation with abdominal visceral fat. Lower abdominal temperature could be a tool for assessment of the visceral fat. Further studies are necessary to uncover relationships between abdominal fat distribution and temperature regulation in obese subjects.
Acknowledgements
This study was supported by Myung-shin Medical Corporation, Gwang-ju, Korea (2011).